

Adjunctive use of hypnosis for clinical pain: a systematic review and meta-analysis
- PMID: 39263007
- PMCID: PMC11390056
- DOI: 10.1097/PR9.0000000000001185
Adjunctive use of hypnosis for clinical pain: a systematic review and meta-analysis
Abstract
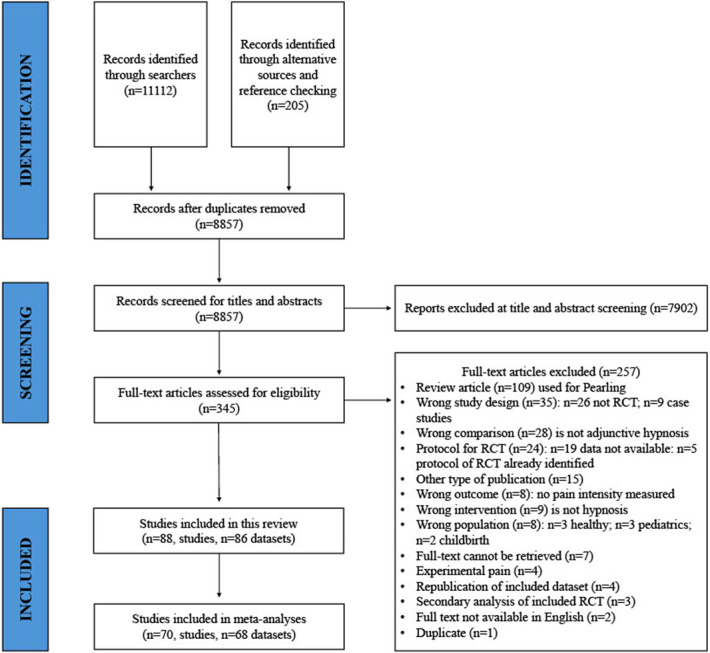
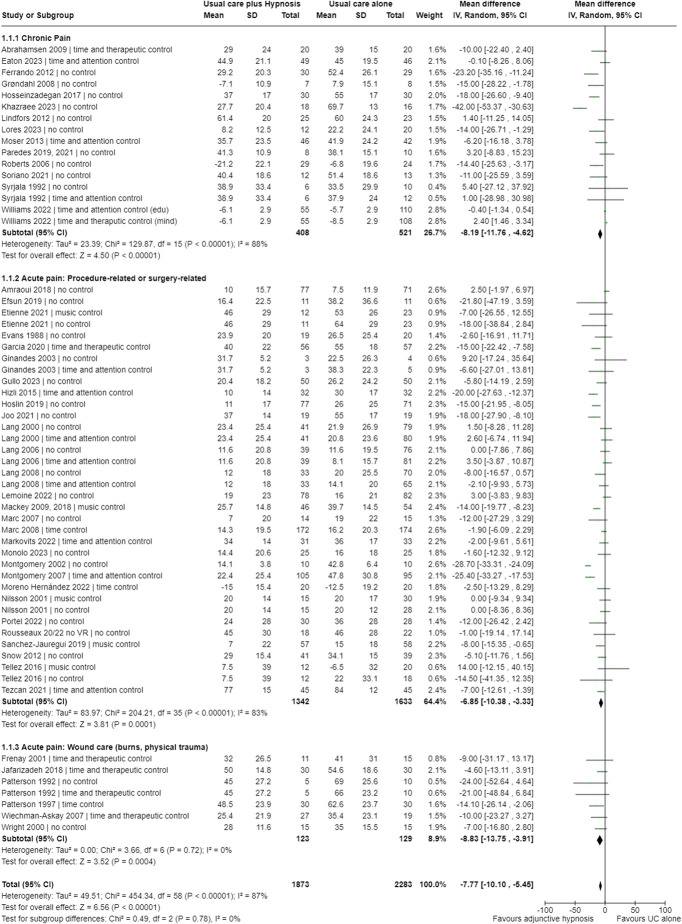
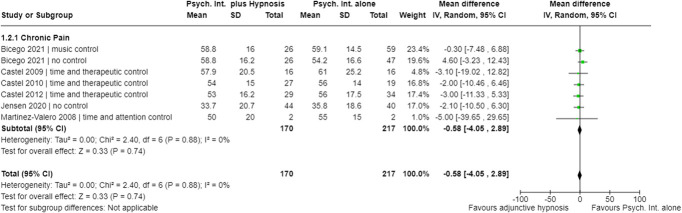
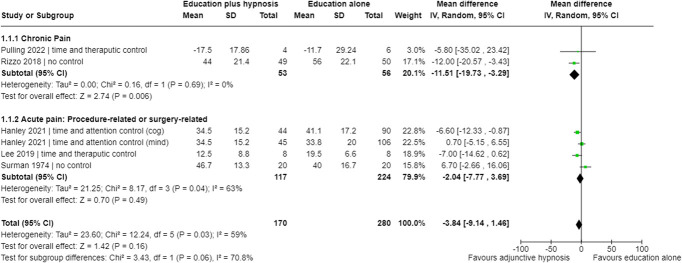
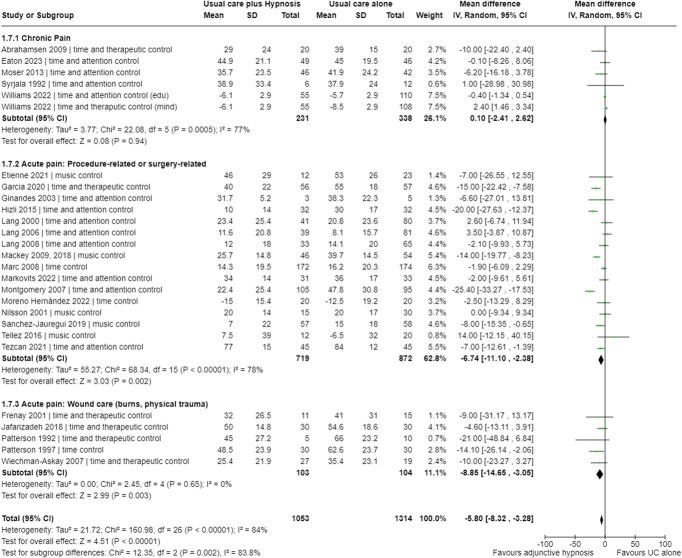
Systematic reviews suggest that stand-alone hypnotic suggestions may improve pain outcomes compared with no treatment, waitlist, or usual care. However, in clinical practice, hypnosis is often provided adjunctively with other interventions, which might have different effects than those reported in previous reviews. This systematic review aimed to summarize the analgesic effects of adjunctive hypnosis in adults with clinical pain. Seven databases (MEDLINE, Embase, PsycINFO, Emcare, SCOPUS, CENTRAL, Cochrane) were searched up to January 2024. Randomised controlled trials comparing the analgesic effects of adjunctive hypnosis (hypnosis + primary intervention) with those of the primary intervention alone were included. Meta-analyses (random-effects model) calculated mean differences (MD, [95% confidence intervals]) for pain intensity (0-100). Seventy studies were pooled in meta-analyses (n = 6078). Hypnosis adjunctive to usual care had a small additional analgesic effect (chronic pain: -8.2 [-11.8, -1.9]; medical procedures/surgical pain: -6.9 [-10.4, -3.3]; burn wound care: -8.8 [-13.8, -3.9]). Hypnosis adjunctive to education had a medium additional analgesic effect for chronic pain (-11.5 [-19.7, 3.3]) but not postsurgery pain (-2.0 [-7.8, 3.7]). When paired with psychological interventions, hypnosis slightly increased analgesia in chronic pain only at the three-month follow-up (-2 [-3.7, -0.3]). Hypnosis adjunctive to medicines had a medium additional analgesic effect for chronic pain (-13.2, [-22.5, -3.8]). The overall evidence certainty is very low; therefore, there is still uncertainty about the analgesic effects of adjunctive hypnosis. However, hypnosis adjunct to education may reduce pain intensity for chronic pain. Clarification of proposed therapeutic targets of adjunctive hypnosis to evaluate underlying mechanisms is warranted.
Keywords: Acute pain; Adjunct; Chronic pain; Hypnosis; Procedural pain; Systematic review.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain.
Conflict of interest statement
R.R.N.R. has received fees from the 2021 Allied Health Cross Boundary Grant Stream to deliver a workshop about pain education and clinical hypnosis. F.A.B. has received support to attend meetings and travel from the International Society for the Study of Pain, the Australian Pain Society, the European Pain Federation, the South Australian Association of Internal Medicine, the Australian Podiatry Association, the Australian Physiotherapy Association, the San Diego Pain Summit, and internal grants from her institutions. G.L.M. has received support from Reality Health, Connect Health, Institutes of Health California, AIA Australia, Workers' Compensation Boards in Australia, Europe and North America, the International Olympic Committee, various professional organisations and learned societies. He receives royalties for several books on pain and speakers' fees for talks on pain and rehabilitation. M.P.J. is the author of 2 books, is the editor of 6 others, and facilitates workshops related to the topic of this paper. He received royalties from the sales of the books and sometimes receives fees for the workshops he facilitates. In addition, M.P.J. owns equity in a company that is developing products to teach hypnosis to individuals to improve their quality of life. T.R.S. has received funding for lectures on pain and rehabilitation and has received royalties for books on pain and rehabilitation. All other authors declare that they have no conflicts of interest.Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures

Similar articles
-
Psychosocial interventions for conversion and dissociative disorders in adults.Cochrane Database Syst Rev. 2020 Jul 17;7(7):CD005331. doi: 10.1002/14651858.CD005331.pub3. Cochrane Database Syst Rev. 2020. PMID: 32681745 Free PMC article.
-
Psychological interventions for needle-related procedural pain and distress in children and adolescents.Cochrane Database Syst Rev. 2018 Oct 4;10(10):CD005179. doi: 10.1002/14651858.CD005179.pub4. Cochrane Database Syst Rev. 2018. PMID: 30284240 Free PMC article.
-
Hypnosis for burn wound care pain and anxiety: A systematic review and meta-analysis.Burns. 2018 Dec;44(8):1870-1881. doi: 10.1016/j.burns.2018.04.017. Epub 2018 May 24. Burns. 2018. PMID: 29803586
-
The effectiveness of hypnotic analgesia in the management of procedural pain in minimally invasive procedures: A systematic review and meta-analysis.J Clin Nurs. 2019 Dec;28(23-24):4207-4224. doi: 10.1111/jocn.15025. Epub 2019 Sep 3. J Clin Nurs. 2019. PMID: 31410922
-
Psychological interventions for people with hemophilia.Cochrane Database Syst Rev. 2020 Mar 18;3(3):CD010215. doi: 10.1002/14651858.CD010215.pub2. Cochrane Database Syst Rev. 2020. PMID: 32187661 Free PMC article.
Cited by
-
The Use of Medical Hypnosis to Prevent and Treat Acute and Chronic Pain: A Systematic Review and Meta-Analysis.J Clin Med. 2025 Jul 1;14(13):4661. doi: 10.3390/jcm14134661. J Clin Med. 2025. PMID: 40649035 Free PMC article. Review.
-
Evaluating Psychological Interventions for Pain, Recovery, and Outcomes in Surgical and Medical Care.Cureus. 2025 Jul 16;17(7):e88097. doi: 10.7759/cureus.88097. eCollection 2025 Jul. Cureus. 2025. PMID: 40821132 Free PMC article. Review.
References
-
- Abrahamsen R, Zachariae R, Svensson P. Effect of hypnosis on oral function and psychological factors in temporomandibular disorders patients. J Oral Rehabil 2009;36:556–70. - PubMed
-
- Adachi T, Fujino H, Nakae A, Mashimo T, Sasaki J. A meta-analysis of hypnosis for chronic pain problems: a comparison between hypnosis, standard care, and other psychological interventions. Int J Clin Exp Hypn 2014;62:1–28. - PubMed
-
- Amraoui J, Pouliquen C, Fraisse J, Dubourdieu J, Rey Dit Guzer S, Leclerc G, de Forges H, Jarlier M, Gutowski M, Bleuse JP, Janiszewski C, Diaz J, Cuvillon P. Effects of a hypnosis session before general anesthesia on postoperative outcomes in patients who underwent minor breast cancer surgery: the HYPNOSEIN randomized clinical trial. JAMA Netw Open. 2018;1:1–13. - PMC - PubMed
-
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003;97:534–40. - PubMed
-
- Aravena V, Garcia FE, Tellez A, Arias PR. Hypnotic intervention in people with fibromyalgia: a randomized controlled trial. Am J Clin Hypn 2020;63:49–61. - PubMed
Publication types
LinkOut - more resources
Full Text Sources