

Syphilis testing, incidence, and reinfection among gay and bisexual men in Australia over a decade spanning HIV PrEP implementation: an analysis of surveillance data from 2012 to 2022
- PMID: 39263009
- PMCID: PMC11387360
- DOI: 10.1016/j.lanwpc.2024.101175
Syphilis testing, incidence, and reinfection among gay and bisexual men in Australia over a decade spanning HIV PrEP implementation: an analysis of surveillance data from 2012 to 2022
Abstract
Background: Gay and bisexual men (GBM) remain overrepresented among syphilis diagnoses in Australia and globally. The extent to which changes in sexual networks associated with HIV pre-exposure prophylaxis (PrEP) and treatment as prevention (TasP) may have influenced syphilis transmission among GBM at the population-level is poorly understood. We describe trends in syphilis testing and incidence among GBM in Australia over eleven years spanning widespread uptake of HIV PrEP and TasP.
Methods: We analysed linked clinical data from GBM aged 16 years or older across a sentinel surveillance network in Australia from January 1, 2012, to December 31, 2022. Individuals with at least two clinic visits and with at least two syphilis tests during the observations period were included in testing and incidence analyses, respectively. Annual rates of testing and infectious syphilis incidence from 2012 to 2022 were disaggregated by HIV status and PrEP use (record of PrEP prescription; retrospectively categorised as ever or never-PrEP user). Cox regression explored associations between demographics, PrEP use and history of bacterial sexually transmissible infections (STIs) and infectious syphilis diagnosis.
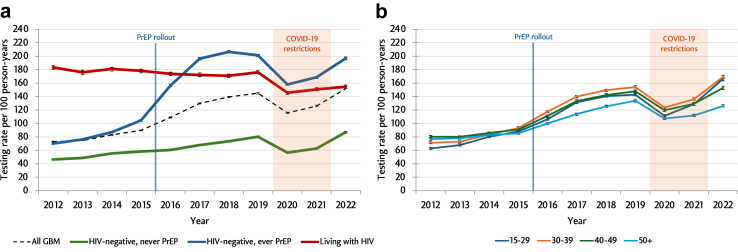
Findings: Among 129,278 GBM (mean age, 34.6 years [SD, 12.2]) included in testing rate analyses, 7.4% were living with HIV at entry and 31.1% were prescribed PrEP at least once during the study period. Overall syphilis testing rate was 114.0/100 person-years (py) and highest among GBM with HIV (168.4/100 py). Syphilis testing increased from 72.8/100 py to 151.8/100 py; driven largely by increases among ever-PrEP users. Among 94,710 GBM included in incidence analyses, there were 14,710 syphilis infections diagnosed over 451,560 person-years (incidence rate = 3.3/100 py). Syphilis incidence was highest among GBM with HIV (6.5/100 py), followed by ever-PrEP users (3.5/100 py) and never-PrEP users (1.4/100 py). From 2012 to 2022, syphilis incidence increased among ever-PrEP users from 1.3/100 py to 5.1/100 py, and fluctuated between 5.4/100 py and 6.6/100 py among GBM with HIV. In multivariable Cox regression, previous syphilis diagnosis (adjusted hazard ratio [aHR] = 1.98, 95% CI = 1.83-2.14), living with HIV (aHR = 1.83, 95% CI = 1.12-1.25) and recent (past 12 m) prescription of PrEP (aHR = 1.78, 95% CI = 1.61-1.97) were associated with syphilis diagnosis.
Interpretation: Syphilis trends between GBM with HIV and GBM with evidence of PrEP use have converged over the past decade in Australia. Our findings recommend targeting emergent syphilis control strategies (e.g. doxycycline post-exposure prophylaxis) to GBM with prior syphilis diagnoses, using HIV PrEP or who are living with HIV.
Funding: Australian Department of Health and Aged Care, National Health and Medical Research Council.
Keywords: Gay and bisexual men; HIV; Incidence; MSM; Men who have sex with men; PrEP; Pre-exposure prophylaxis; Surveillance; Syphilis; Treatment as prevention; Treponema pallidum.
© 2024 The Author(s).
Conflict of interest statement
M.W.T. reports speakers’ honoraria, consultancy fees and investigator-initiated research grants from Gilead Sciences. R.G. has received research support funding from Cepheid and SpeeDx. M.E.H. reports investigator-initiated research grants from Gilead Sciences and Abbvie outside of the submitted work. M.A.S. reports investigator-initiated research grants from Gilead Sciences and Abbvie and consulting fees from Gilead Sciences outside of the submitted work. M.B. reports medical advisory boards and speakers’ honoraria from Gilead Sciences and ViiV Healthcare, and funding to attend scientific meetings from Gilead Sciences, investigator-initiated research grants from ViiV Healthcare. EPFC is supported by an Australian National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (GNT1172873), and has received speakers’ honoraria from Gilead Sciences, MSD and CSL Seqirus. CKF is supported by an Australian NHMRC Leadership Investigator Grant (GNT1172900). VC received payment from Gilead Science for participation on advisory board. DO is CEO of Health Equity Matters, Australia's peak community HIV organization, for part of the period during which the research was undertaken. All other authors declare no conflicts of interest.
Figures

References
-
- Jasek E., Chow E.P., Ong J.J., et al. Sexually transmitted infections in Melbourne, Australia from 1918 to 2016: nearly a century of data. Commun Dis Intell Q Rep. 2017;41(3):E212–E222. - PubMed
-
- Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030. 2022.
-
- Fourth national sexually transmissible infections strategy. 2019. https://www1.health.gov.au/internet/main/publishing.nsf/Content/ohp-bbvs... - PubMed
-
- Donovan B., Dayan L. In: Oxford textbook of medicine. Warrell D.A., Cox T.M., Firth J.D., editors. Oxford University Press; Oxford: 2010. Syphilis; pp. 885–896.
LinkOut - more resources
Full Text Sources
Miscellaneous
