

LungPath: artificial intelligence-driven histologic pattern recognition for improved diagnosis of early-stage invasive lung adenocarcinoma
- PMID: 39263012
- PMCID: PMC11384487
- DOI: 10.21037/tlcr-24-258
LungPath: artificial intelligence-driven histologic pattern recognition for improved diagnosis of early-stage invasive lung adenocarcinoma
Abstract
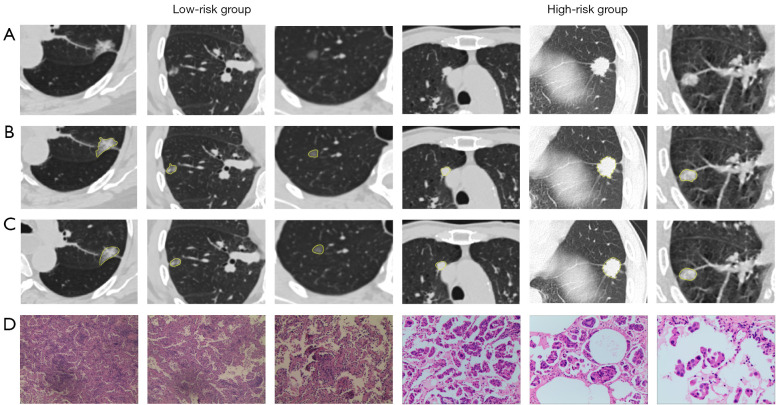
Background: Early-stage invasive lung adenocarcinoma (ADC) characterized by a predominant micropapillary or solid pattern exhibit an elevated risk of recurrence following sub-lobar resection, thus determining histological subtype of early-stage invasive ADC prior surgery is important for formulating lobectomy or sub-lobar resection. This study aims to develop a deep learning algorithm and assess its clinical capability in distinguishing high-risk or low-risk histologic patterns in early-stage invasive ADC based on preoperative computed tomography (CT) scans.
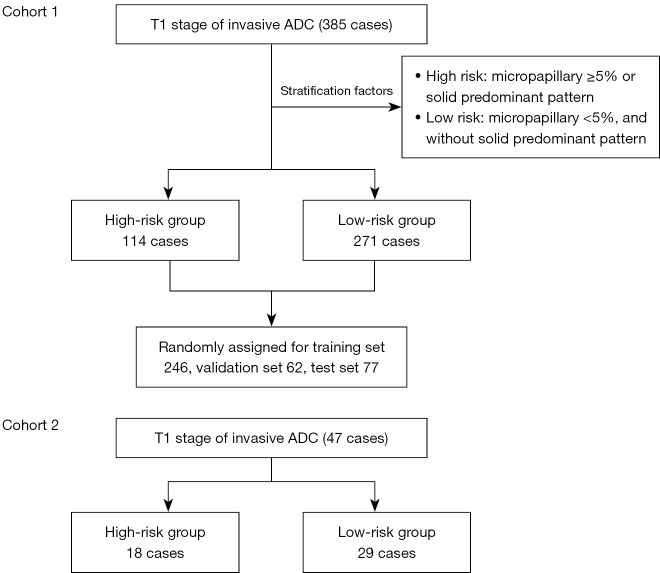
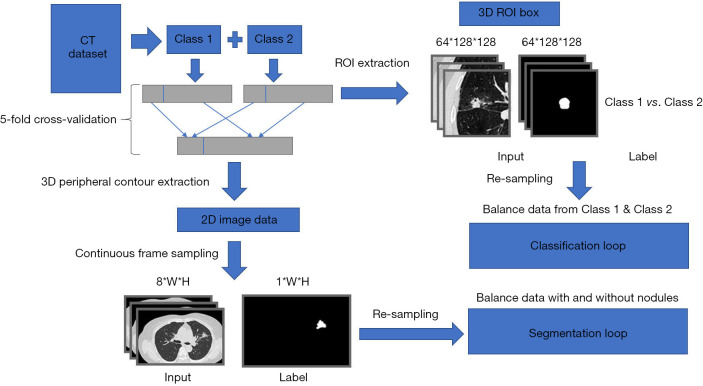
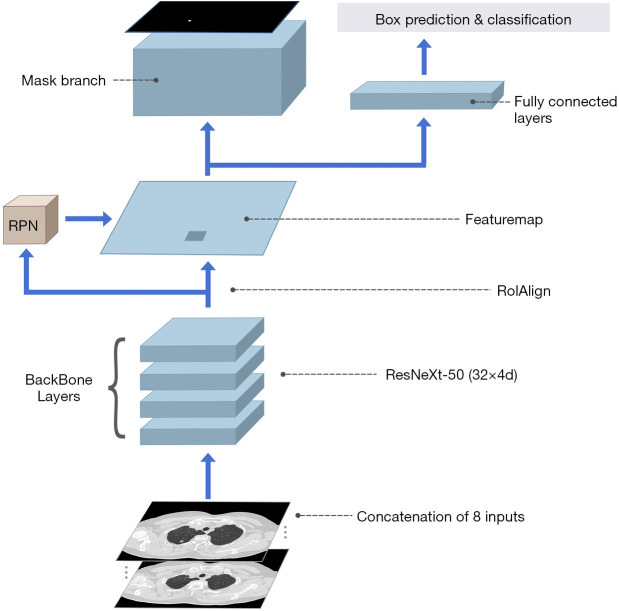
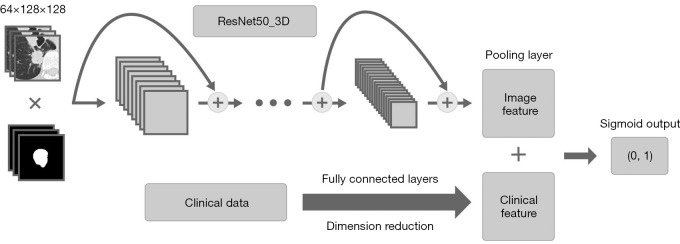
Methods: Two retrospective cohorts were included: development cohort 1 and external test cohort 2, comprising patients diagnosed with T1 stage invasive ADC. Electronic medical records and CT scans of all patients were documented. Patients were stratified into two risk groups. High-risk group: comprising cases with a micropapillary component ≥5% or a predominant solid pattern. Low-risk group: encompassing cases with a micropapillary component <5% and an absence of a predominant solid pattern. The overall segmentation model was modified based on Mask Region-based Convolutional Neural Network (Mask-RCNN), and Residual Network 50 (ResNet50)_3D was employed for image classification.
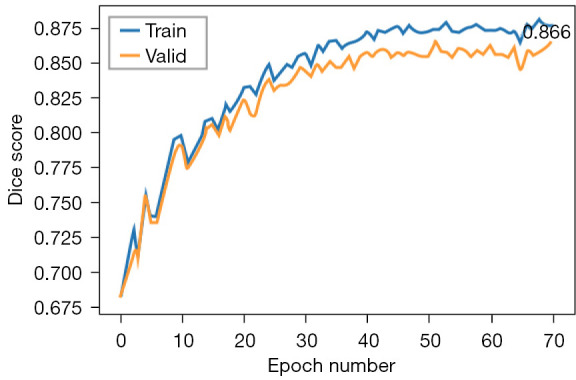
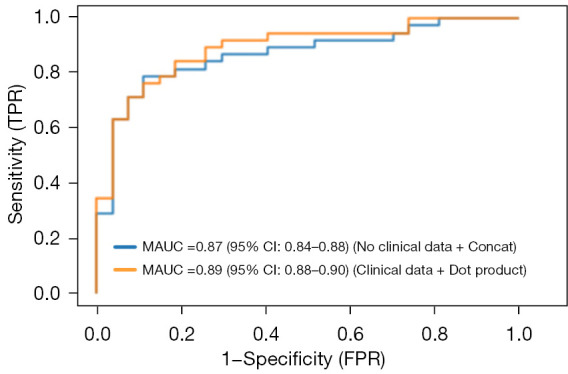
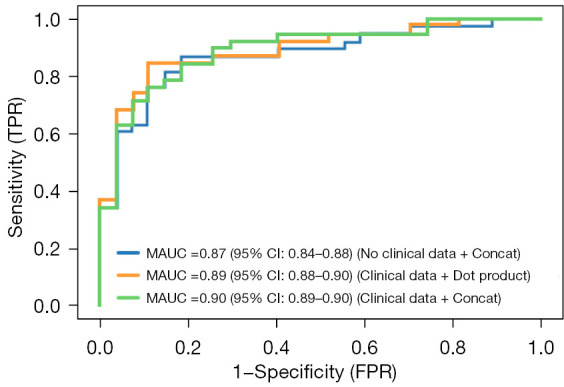
Results: A total of 432 patients participated in this study, with 385 cases in cohort 1 and 47 cases in cohort 2. The fine-outline results produced by the auto-segmentation model exhibited a high level of agreement with manual segmentation by human experts, yielding a mean dice coefficient of 0.86 [95% confidence interval (CI): 0.85-0.87] in cohort 1 and 0.84 (95% CI: 0.82-0.85) in cohort 2. Furthermore, the deep learning model effectively differentiated the high-risk group from the low-risk group, achieving an area under the curve (AUC) of 0.89 (95% CI: 0.88-0.90) in cohort 1. In the external validation conducted in cohort 2, the deep learning model displayed an AUC of 0.87 (95% CI: 0.84-0.88) in distinguishing the high-risk group from the low-risk group. The average diagnostic time was 16.00±3.2 seconds, with an accuracy of 0.82 (95% CI: 0.81-0.83).
Conclusions: We have developed a deep learning algorithm, LungPath, for the automated segmentation of pulmonary nodules and prediction of high-risk histological patterns in early-stage lung ADC based on CT scans.
Keywords: Artificial intelligence (AI); early-stage invasive lung adenocarcinoma (early-stage invasive lung ADC); histologic patterns.
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-258/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources