

Risk prediction of postoperative permanent stroke in acute type A aortic dissection patients with severe common carotid artery stenosis using brain CT perfusion
- PMID: 39263105
- PMCID: PMC11386277
- DOI: 10.1016/j.heliyon.2024.e36740
Risk prediction of postoperative permanent stroke in acute type A aortic dissection patients with severe common carotid artery stenosis using brain CT perfusion
Abstract
Rationale and objectives: To explore the feasibility and predictive utility for neurological outcomes of brain computed tomography perfusion (CTP) for surgically treated acute type A aortic dissection patients with severe common carotid artery stenosis.
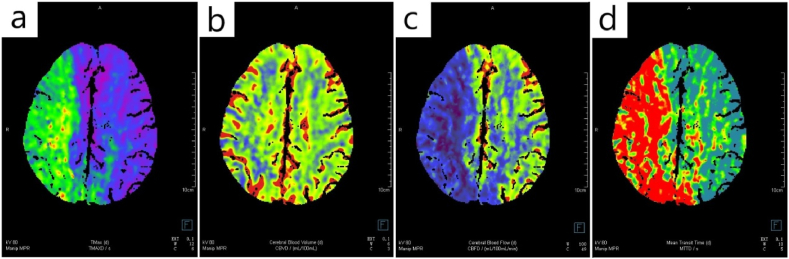
Materials and methods: Consecutive acute type A aortic dissection patients with severe common carotid artery stenosis undergoing preoperative brain computed tomography perfusion and surgery at our center were examined in retrospect. Brain perfusion was assessed using parameters including cerebral blood flow, cerebral blood volume, mean transmit time, time to maximum, penumbra volume and infarct core volume. Univariable and multivariable regression analyses were performed to identify clinical and imaging predictors associated with postoperative permanent stroke.
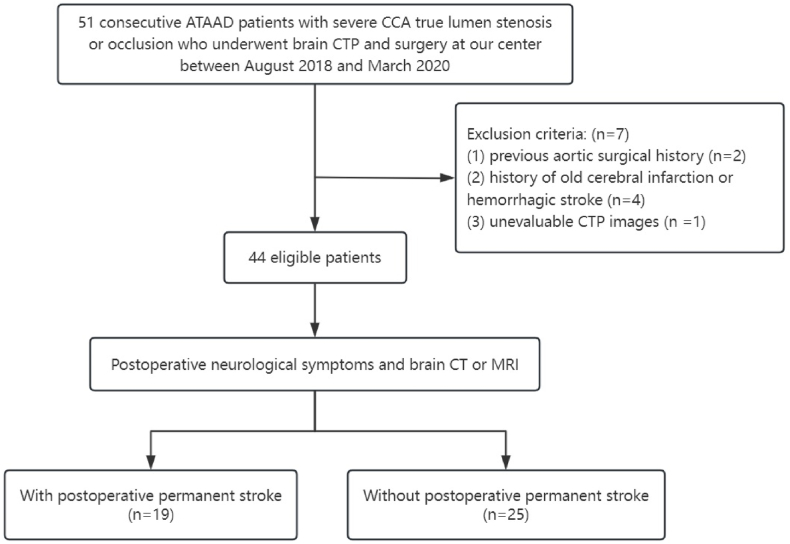
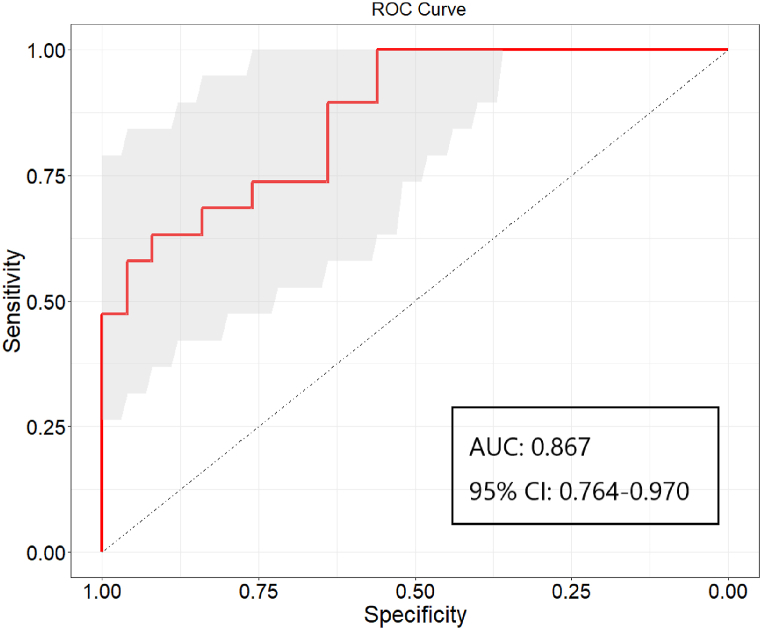
Results: Out of 44 patients included, 19 patients (43.2 %) presented with postoperative permanent stroke. Univariable analysis revealed that internal carotid artery dissection, cerebral blood flow of the affected side, cerebral blood volume of the affected side, and penumbra volume were implicated in postoperative permanent stroke. Multivariable analysis further showed that cerebral blood flow of the affected side was an independent indicator of a permanent stroke following surgery (odds ratio: 0.820, 95 % confidence interval: 0.684-0.982; p = 0.012). The area under the receiver operating characteristic curve was 0.867 (95 % confidence interval: 0.764-0.970), and the optimal cut-off value was 45.6mL/100 mL/min.
Conclusion: Cerebral blood flow of the affected side was an independent indicator of permanent stroke following surgery in acute type A aortic dissection patients with severe common carotid artery stenosis. Brain CTP could be a helpful modality for quantitative evaluation of cerebral malperfusion and neurological prognostication.
Keywords: Acute aortic dissection; Cerebral malperfusion; Computed tomography perfusion; Permanent stroke; Risk prediction.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Neurological prognosis in surgically treated acute aortic dissection with brain computed tomography perfusion.Eur J Cardiothorac Surg. 2024 Jan 2;65(1):ezad437. doi: 10.1093/ejcts/ezad437. Eur J Cardiothorac Surg. 2024. PMID: 38175783
-
Novel brain computed tomography perfusion for cerebral malperfusion secondary to acute type A aortic dissection.Interact Cardiovasc Thorac Surg. 2022 Jun 15;35(1):ivac046. doi: 10.1093/icvts/ivac046. Interact Cardiovasc Thorac Surg. 2022. PMID: 35218663 Free PMC article.
-
Impact of direct carotid artery perfusion in acute type A aortic dissection involving the common carotid artery.Gen Thorac Cardiovasc Surg. 2021 Nov;69(11):1467-1475. doi: 10.1007/s11748-021-01628-y. Epub 2021 Apr 2. Gen Thorac Cardiovasc Surg. 2021. PMID: 33797692 Free PMC article.
-
Perfusion computed tomography thresholds defining ischemic penumbra and infarct core: studies in a rat stroke model.Int J Stroke. 2015 Jun;10(4):553-9. doi: 10.1111/ijs.12147. Epub 2013 Oct 21. Int J Stroke. 2015. PMID: 24138577
-
Extension of therapeutic window in ischemic stroke by selective mismatch imaging.Int J Stroke. 2019 Jun;14(4):351-358. doi: 10.1177/1747493019840936. Epub 2019 Apr 1. Int J Stroke. 2019. PMID: 30935350 Review.
References
-
- Morimoto N., Okada K., Okita Y. Lack of neurologic improvement after aortic repair for acute type A aortic dissection complicated by cerebral malperfusion: predictors and association with survival. J. Thorac. Cardiovasc. Surg. 2011;142(6):1540–1544. - PubMed
-
- Di Eusanio M., Patel H.J., Nienaber C.A., et al. Patients with type A acute aortic dissection presenting with major brain injury: should we operate on them? J. Thorac. Cardiovasc. Surg. 2013;145(3 Suppl):S213–S221.e1. - PubMed
-
- Bossone E., Corteville D.C., Harris K.M., et al. Stroke and outcomes in patients with acute type A aortic dissection. Circulation. 2013;128(11 Suppl 1):S175–S179. - PubMed
-
- Sultan I., Bianco V., Patel H.J., et al. Surgery for type A aortic dissection in patients with cerebral malperfusion: results from the international registry of acute aortic dissection. J. Thorac. Cardiovasc. Surg. 2021;161(5):1713–1720.e1. - PubMed
-
- Fukuhara S., Norton E.L., Chaudhary N., et al. Type A aortic dissection with cerebral malperfusion: new insights. Ann. Thorac. Surg. 2021;112(2):501–509. - PubMed
LinkOut - more resources
Full Text Sources
