

Multicenter, propensity-weighted comparison of stented, rapid-deployment and new-generation aortic valves
- PMID: 39263409
- PMCID: PMC11387204
- DOI: 10.1016/j.ijcha.2024.101487
Multicenter, propensity-weighted comparison of stented, rapid-deployment and new-generation aortic valves
Abstract
Background: Conventional stented, rapid deployment and new-generation stented valves are now available for surgical aortic valve replacement (SAVR). New-generation devices feature advanced tissue treatment for theoretical prolonged durability and a new stent design able to expand in case of future transcatheter Valve-in-Valve. Aim of this retrospective, multicenter, propensity-weighted study was to compare early clinical and hemodynamic outcomes of these three different bioprostheses.
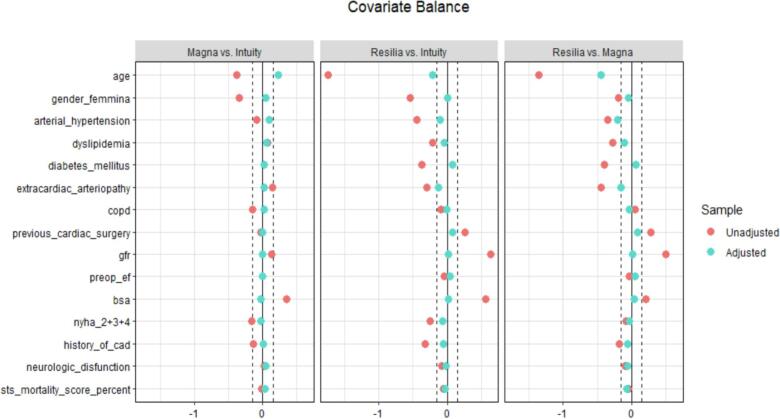
Methods: We analyzed data of 2589 patients from two national multicenter registries and one Institutional database. Study devices were Magna Ease, Intuity/Intuity Elite and Inspiris Resilia (Edwards Lifesciences, Irvine, CA, USA) and were implanted in 296 (11.4 %), 1688 (65.2 %) and 605 (23.4 %) patients, respectively. A propensity score weighting approach was employed.
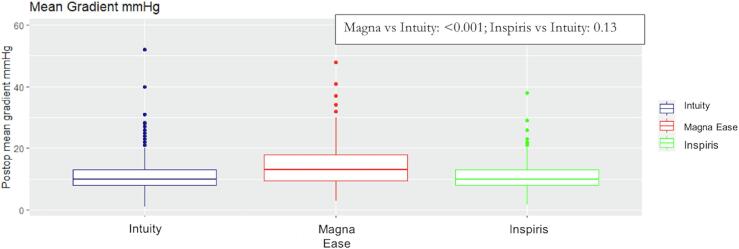
Results: In isolated SAVR, aortic cross clamp (ACC) time was shorter for Intuity (Magna Ease: 87, Intuity: 55, Inspiris: 70 min; Magna Ease vs. Intuity: p < 0.001; Inspiris vs. Intuity: p < 0.001). Overall mortality was 2 %, 1.7 % and 0.5 % in Magna Ease, Intuity and Inspiris groups, respectively (Magna Ease vs. Intuity: p = 0.476; Inspiris vs. Intuity: p = 0.395); permanent pace-maker implantation rate was lower for Inspiris (Magna Ease: 6 %, Intuity: 6 %, Inspiris: 2 %; Magna Ease vs. Intuity: p = 0.679; Inspiris vs. Intuity: p < 0.001). Median mean gradients were 13, 10 and 10 mmHg for Magna Ease, Intuity and Inspiris, respectively (Magna Ease vs. Intuity: p < 0.001; Inspiris vs. Intuity: p = 0.13).
Conclusions: All study devices provide excellent early clinical and hemodynamic outcomes. Inspiris shows low rates of permanent pace-maker implantation and its transaortic gradients are similar to rapid-deployment valves and lower than Magna Ease.
Keywords: Aortic valve replacement; Bioprostheses; Rapid-deployment aortic bioprostheses; Stented aortic bioprosthesis.
© 2024 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Augusto D’Onofrio reports a relationship with Edwards that includes: speaking and lecture fees and travel reimbursement. Giorgia Cibin reports a relationship with Edwards Lifesciences Corporation that includes: funding grants. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Isaacs A.J., Shuhaiber J., Salemi A., Isom O.W., Sedrakyan A. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J. Thorac. Cardiovasc. Surg. 2015;149:1262–1269. - PubMed
-
- Fujita B., Ensminger S., Bauer T., Möllmann H., Beckmann A., Bekeredjian R., et al. Trends in practice and outcomes from 2011 to 2015 for surgical aortic valve replacement: an update from the German Aortic Valve Registry on 42 776 patients. Eur. J. Cardiothorac. Surg. 2018;53:552–559. - PubMed
-
- Siregar S., de Heer F., Groenwold R.H., Versteegh M.I., Bekkers J.A., Brinkman E.S., et al. Trends and outcomes of valve surgery: 16-year results of Netherlands Cardiac Surgery National Database. Eur. J. Cardiothorac. Surg. 2014;46:386–397. - PubMed
-
- Dunning J., Gao H., Chambers J., Moat N., Murphy G., Pagano D., et al. Aortic valve surgery: marked increases in volume and significant decreases in mechanical valve use–an analysis of 41,227 patients over 5 years from the Society for Cardiothoracic Surgery in Great Britain and Ireland National database. J. Thorac. Cardiovasc. Surg. 2011;142:776–782. - PubMed
-
- Schnittman S.R., Adams D.H., Itagaki S., Toyoda N., Egorova N.N., Chikwe J. Bioprosthetic aortic valve replacement: Revisiting prosthesis choice in patients younger than 50 years old. J. Thorac. Cardiovasc. Surg. 2018;155:539–547. - PubMed
LinkOut - more resources
Full Text Sources
