

Device Closure of Hemodynamically Significant Patent Ductus Arteriosus in Premature Infants
- PMID: 39263415
- PMCID: PMC11388744
- DOI: 10.1016/j.jacadv.2024.101211
Device Closure of Hemodynamically Significant Patent Ductus Arteriosus in Premature Infants
Abstract
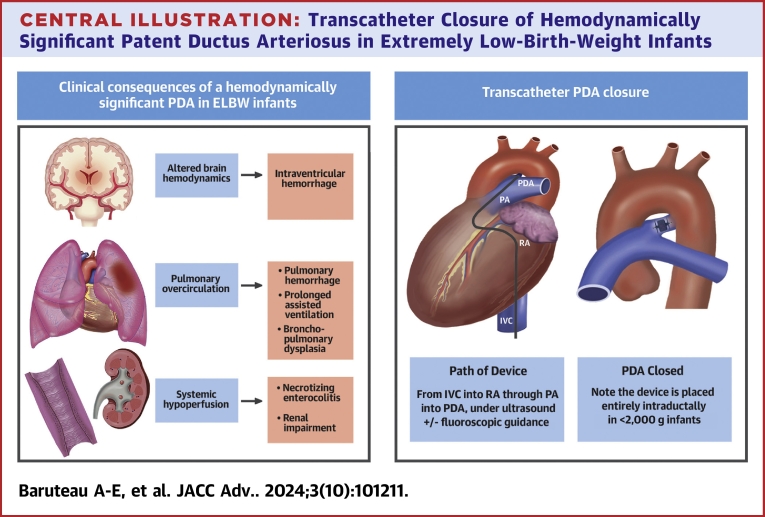
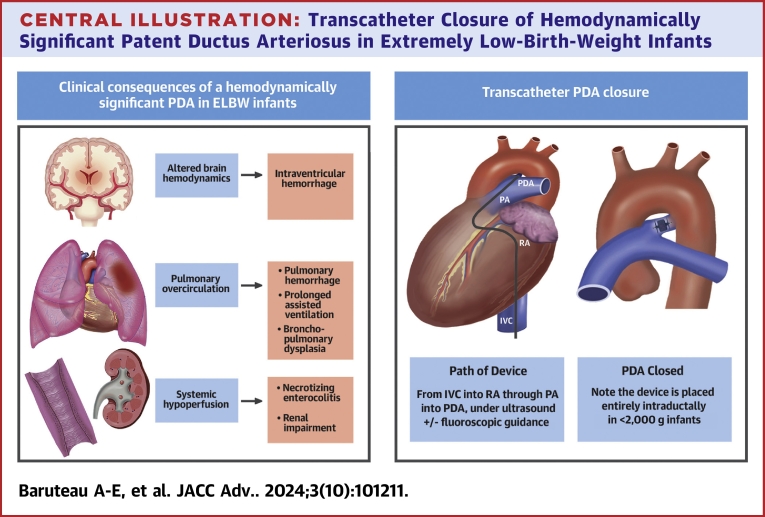
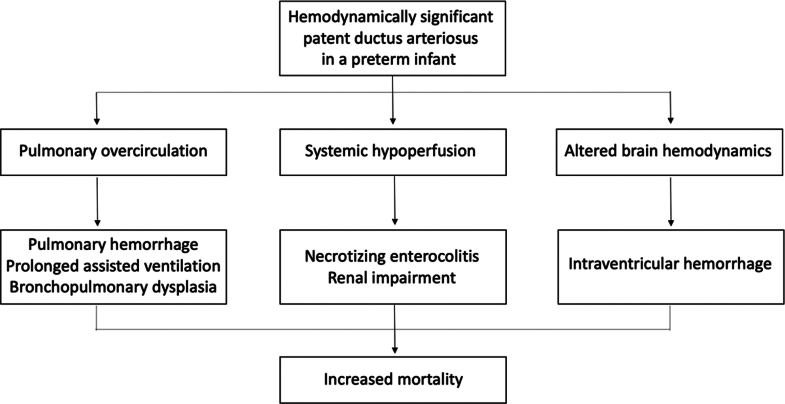
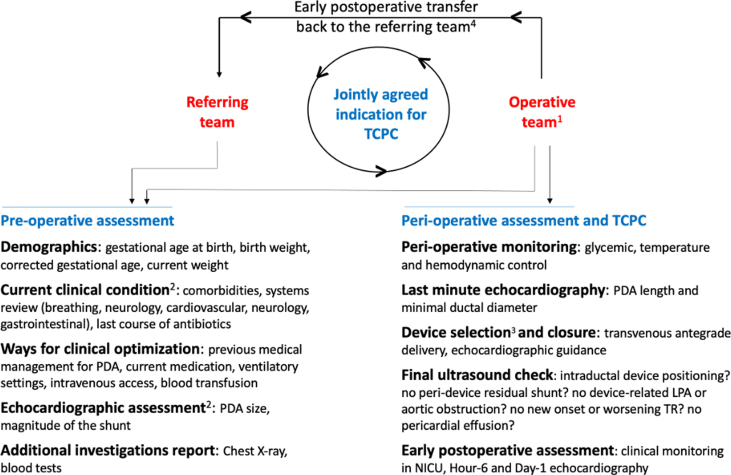
The patent ductus arteriosus is a very common condition in preterm infants, and a hemodynamically significant patent ductus arteriosus increases morbidity and mortality in these vulnerable patients. However, despite numerous randomized controlled trials, there is no consensus regarding management. Medical therapy is typically offered as first-line treatment, although it yields limited success and carries the potential for severe adverse events. In recent years, there has been rapid development in transcatheter patent ductus arteriosus closure primary with the use of the Amplatzer Piccolo Occluder, and this has gained widespread acceptance as a safe and effective alternative to surgical ligation in extremely low-birth-weight infants weighing over 700 g. This article aims to provide an appraisal of the patient selection process, a step-by-step procedural guide, and a comprehensive review of the outcomes associated with this approach.
Keywords: echocardiography; extremely low birth weight infants; outcomes; patent ductus arteriosus; premature infant.
© 2024 The Authors.
Conflict of interest statement
Dr Alban-Elouen Baruteau is supported by the French Government as part of the “Investments of the Future” program managed by the National Research Agency (grant reference ANR-16-IDEX-0007); and is a consultant and proctor for Abbott. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Hundscheid T., Onland W., Kooi E.M.W., et al. Expectant management or early ibuprofen for patent ductus arteriosus. N Engl J Med. 2023;388:980–990. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
