

Sex differences in mobility recovery after hip fracture: a time series analysis
- PMID: 39263423
- PMCID: PMC11390126
- DOI: 10.3389/fpubh.2024.1434182
Sex differences in mobility recovery after hip fracture: a time series analysis
Abstract
Introduction: Sex differences are commonly reported for hip fracture incidence rates and recovery. Current knowledge about mobility recovery after hip fracture involves clinical assessments of physical capacity or patient-reported outcomes. Information on mobility performance during daily life is missing but relevant to evaluate patients' recovery. Hence, it remains unclear whether sex differences exist in the longitudinal progression of mobility performance in hip fracture patients. To investigate this, we pooled data from four studies in Germany and Norway.
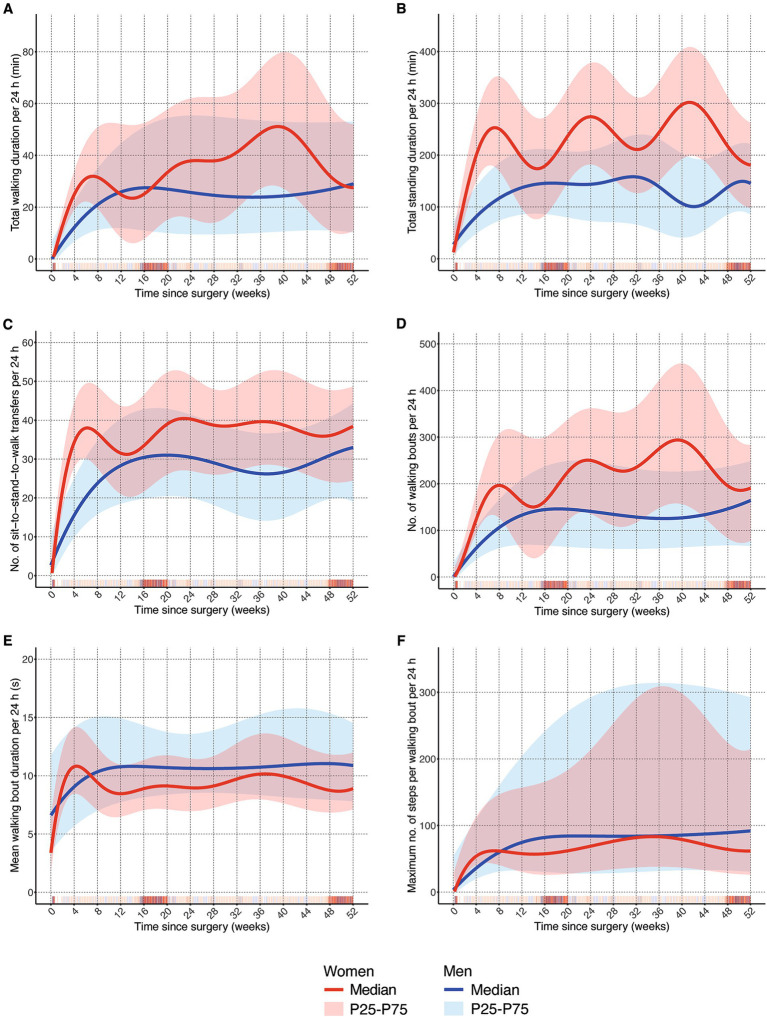
Methods: In all studies, real-world mobility was assessed continuously over 1 to 7 days using a sensor fixed to the unaffected frontal thigh. All studies assessed mobility at different time points that were allocated to three distinct phases: Acute and post-acute phase (week 1-6), extended recovery (7-26), and long-term recovery (27-52). Sex-specific continuous trajectories of the median (50th percentile) as well as the 1st (25th percentile) and 3rd quartile (75th percentile) were estimated using quantile regression models with splines for daily walking and standing duration; number of sit-to-stand-to-walk transfers and walking bouts; mean walking bout duration; maximum number of steps per walking bout.
Results: There were 5,900 valid observation days from n = 717 participants (mean age = 83.4 years, SD 6.1). The majority was female (75.3%), with similar sex distribution across all studies. Demographics of both sexes were comparable, but a higher percentage of women was living alone (69.0% compared to 40.9% in men) and had experienced an indoor fall leading to the fracture (74.3% compared to 67.4% in men). There were clear sex differences in mobility recovery. Women improved their mobility faster than men, but men showed larger increases later in the year after surgery. At the end of the first year, both sexes reached comparable levels in almost all mobility parameters.
Conclusion: We identified varying aspects of mobility recovery between men and women, i.e., timely development of mobility recovery shows different patterns. Our findings support the consideration of sex differences in planning and implementing rehabilitation measures for hip fracture patients and highlight the need to provide adapted support at different time points. The underlying mechanisms of these sex differences need further investigation.
Keywords: digital mobility outcomes; hip fracture; mobility; real-world walking; sex differences.
Copyright © 2024 Jansen, Engdal, Peter, Helbostad, Taraldsen, Vereijken, Pfeiffer, Becker and Klenk.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Moerman S, Mathijssen NM, Tuinebreijer WE, Nelissen RG, Vochteloo AJ. Less than one-third of hip fracture patients return to their prefracture level of instrumental activities of daily living in a prospective cohort study of 480 patients. Geriatr Gerontol Int. (2018) 18:1244–8. doi: 10.1111/ggi.13471 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical