

Comparing outcomes after pulmonary vein isolation in patients with systolic and diastolic heart failure
- PMID: 39263616
- PMCID: PMC11385397
- DOI: 10.1016/j.hroo.2024.07.003
Comparing outcomes after pulmonary vein isolation in patients with systolic and diastolic heart failure
Abstract
Background: The benefit of pulmonary vein isolation (PVI) in patients with atrial fibrillation (AF) and heart failure with reduced ejection fraction (HFrEF) is well established; its efficacy in patients with heart failure preserved ejection fraction (HFpEF) is less clear.
Objective: The objective of the study was to compare AF and heart failure (HF) rehospitalizations after PVI in patients with HFpEF vs HFrEF.
Methods: The IBM MarketScan Database was used to identify patients undergoing PVI for AF. Patients were categorized by HF status: absence of HF, presence of HFrEF, or presence of HFpEF. Primary outcomes were HF and arrhythmia hospitalizations after PVI.
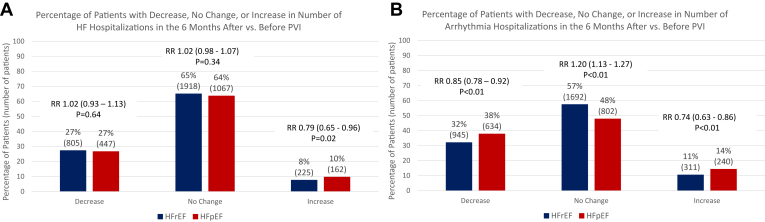
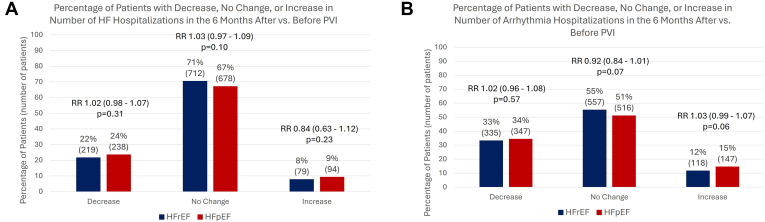
Results: A total of 32,524 patients were analyzed: 27,900 with no HF (86%), 2948 with HFrEF (9%), and 1676 with HFpEF (5%). Compared with those with no HF, both patients with HFrEF and HFpEF were more likely to be hospitalized for HF (hazard ratio [HR] 7.27; P < .01 for HFrEF and HR 9.46; P < .01 for HFpEF) and for AF (HR 1.17; P < .01 for HFrEF and HR 1.74; P < .01 for HFpEF) after PVI. In matched analysis, 23% of patients with HFrEF and 24% patients with HFpEF demonstrated a reduction in HF hospitalizations (P = .31) and approximately one-third demonstrated decreased arrhythmia rehospitalizations (P = .57) in the 6 months after PVI. Compared with those with HFrEF in longer-term follow-up (>1 year), patients with HFpEF were more likely to have HF (HR 1.30; P < .01) and arrhythmia (HR 1.19; P < .01) rehospitalizations.
Conclusion: Reductions in HF and arrhythmia hospitalizations are observed early after PVI across all patients with HF, but patients with HFpEF demonstrate higher HF rehospitalization and arrhythmia recurrence in longer-term follow-up than do patients with HFrEF.
Keywords: Atrial fibrillation; Diastolic dysfunction; Heart failure with preserved ejection fraction; Heart failure with reduced ejection fraction; Pulmonary vein isolation.
© 2024 Heart Rhythm Society. Published by Elsevier Inc.
Figures



References
-
- Hindricks G., Potpara T., Kirchhof P., et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. - PubMed
-
- Joglar J.A., Chung M.K., Armbruster A.L., et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:E1–E156. - PMC - PubMed
-
- Di Biase L., Mohanty P., Mohanty S., et al. Ablation versus amiodarone for treatment of persistent atrial fibrillation in patients with congestive heart failure and an implanted device: results from the AATAC multicenter randomized trial. Circulation. 2016;133:1637–1644. - PubMed
-
- Prabhu S., Taylor A.J., Costello B.T., et al. Catheter ablation versus medical rate control in atrial fibrillation and systolic dysfunction: the CAMERA-MRI study. J Am Coll Cardiol. 2017;70:1949–1961. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
