

Brain perfusion SPECT in the presurgical evaluation of epilepsy: is additional ictal SPECT required in case of high-confidence lateralization of the seizure onset zone by interictal SPECT and vice versa?
- PMID: 39264384
- PMCID: PMC11393367
- DOI: 10.1186/s13550-024-01149-8
Brain perfusion SPECT in the presurgical evaluation of epilepsy: is additional ictal SPECT required in case of high-confidence lateralization of the seizure onset zone by interictal SPECT and vice versa?
Abstract
Background: Ictal brain perfusion SPECT provides higher sensitivity for the identification of the epileptic seizure onset zone (SOZ) than interictal SPECT. However, ictal SPECT is demanding due to the unpredictable waiting period for the next seizure to allow for ictal tracer injection. Thus, starting with an interictal scan and skipping the ictal scan if the interictal scan provides a SOZ candidate with high confidence could be an efficient approach. The current study estimated the rate of high-confidence SOZ candidates and the false lateralization rate among them for interictal and ictal SPECT.
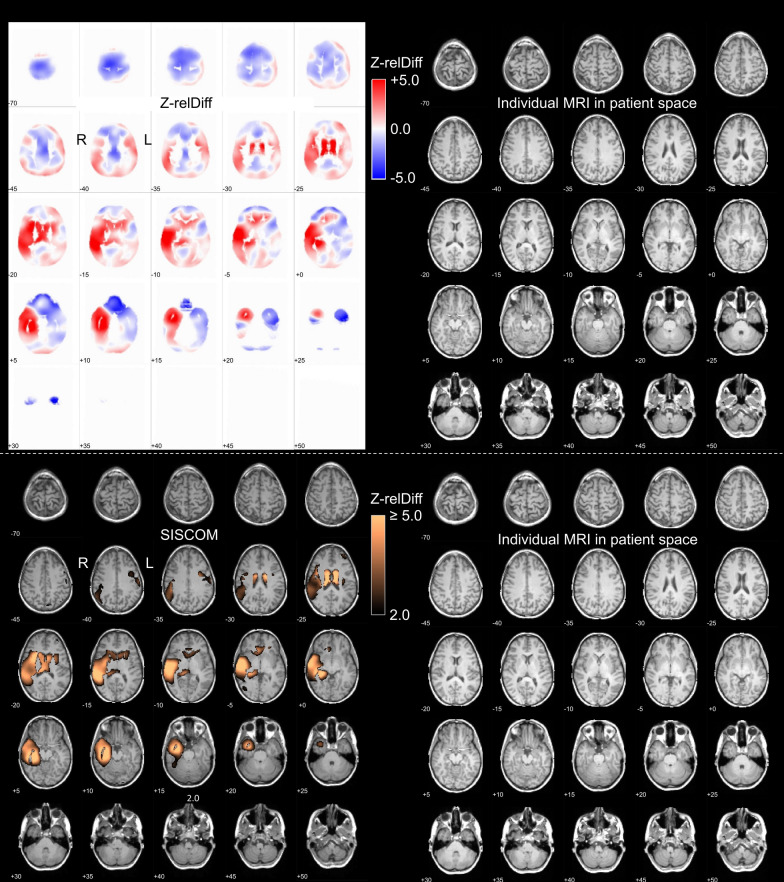
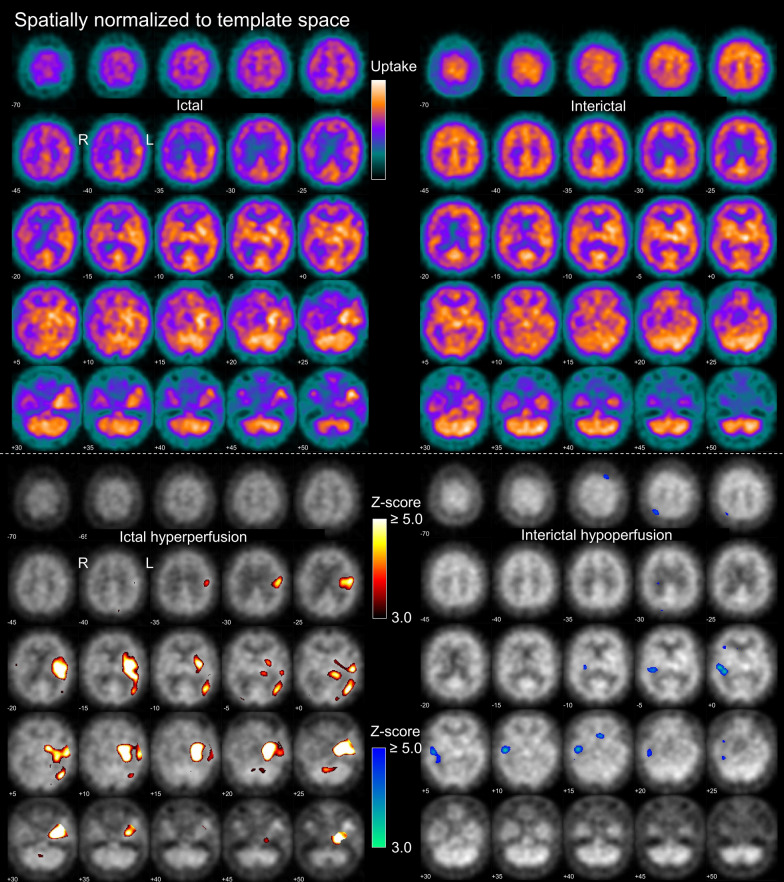
Methods: 177 patients (48% females, median age 38y, interquartile range 27-48y) with ictal and interictal SPECT acquired with 99mTc-HMPAO (n = 141) or -ECD (n = 36) were included retrospectively. The vast majority of the patients was suspected to have temporal lobe epilepsy. Visual interpretation of the SPECT data was performed independently by 3 readers in 3 settings: "interictal only" (interictal SPECT and statistical hypoperfusion map), "ictal only" (ictal SPECT and hyperperfusion map), and "full" setting (side-by-side interpretation of ictal and interictal SPECT including statistical maps and SISCOM analysis). The readers lateralized the SOZ (right, left, none) and characterized their confidence using a 5-score. A case was considered "lateralizing with high confidence" if all readers lateralized to the same hemisphere with at least 4 of 5 confidence points. Lateralization of the SOZ in the "full" setting was used as reference standard.
Results: The proportion of "lateralizing with high confidence" cases was 4.5/31.6/38.4% in the "interictal only"/"ictal only"/"full" setting. One (12.5%) of the 8 cases that were "lateralizing with high confidence" in the "interictal only" setting lateralized to the wrong hemisphere. Among the 56 cases that were "lateralizing with high confidence" in the "ictal only" setting, 54 (96.4%) were also lateralizing in the "full" setting, all to the same hemisphere.
Conclusions: Starting brain perfusion SPECT in the presurgical evaluation of epilepsy with an interictal scan to skip the ictal scan in case of a high-confidence interictal SOZ candidate is not a useful approach. In contrast, starting with an ictal scan to skip the interictal scan in case of a high-confidence ictal SOZ candidate can be recommended.
Keywords: 99mTc-ECD; 99mTc-HMPAO; Cerebral blood flow; Epilepsy; Ictal; Interictal; Perfusion; SISCOM; SPECT; Seizure onset zone.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Leveille J, Demonceau G, De Roo M, Rigo P, Taillefer R, Morgan RA, et al. Characterization of technetium-99m-L, L-ECD for brain perfusion imaging, Part 2: biodistribution and brain imaging in humans. J Nucl Med. 1989;30:1902–10. - PubMed
-
- Walovitch RC, Hill TC, Garrity ST, Cheesman EH, Burgess BA, O’Leary DH, et al. Characterization of technetium-99m-L, L-ECD for brain perfusion imaging, Part 1: pharmacology of technetium-99m ECD in nonhuman primates. J Nucl Med. 1989;30:1892–901. - PubMed
-
- Vallabhajosula S, Zimmerman RE, Picard M, Stritzke P, Mena I, Hellman RS, et al. Technetium-99m ECD: a new brain imaging agent: in vivo kinetics and biodistribution studies in normal human subjects. J Nucl Med. 1989;30:599–604. - PubMed
-
- Sharp PF, Smith FW, Gemmell HG, Lyall D, Evans NT, Gvozdanovic D, et al. Technetium-99m HM-PAO stereoisomers as potential agents for imaging regional cerebral blood flow: human volunteer studies. J Nucl Med. 1986;27:171–7. - PubMed
-
- Neirinckx RD, Canning LR, Piper IM, Nowotnik DP, Pickett RD, Holmes RA, et al. Technetium-99m d, l-HM-PAO: a new radiopharmaceutical for SPECT imaging of regional cerebral blood perfusion. J Nucl Med. 1987;28:191–202. - PubMed
LinkOut - more resources
Full Text Sources
