

Treatment patterns and burden of infection in patients with chronic lymphocytic leukemia and secondary immunodeficiency: a retrospective database study
- PMID: 39264434
- PMCID: PMC11534992
- DOI: 10.1007/s00277-024-05984-6
Treatment patterns and burden of infection in patients with chronic lymphocytic leukemia and secondary immunodeficiency: a retrospective database study
Abstract
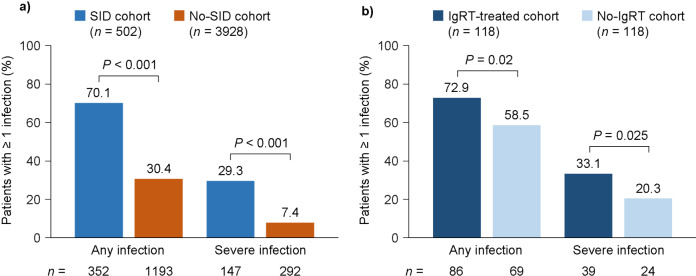
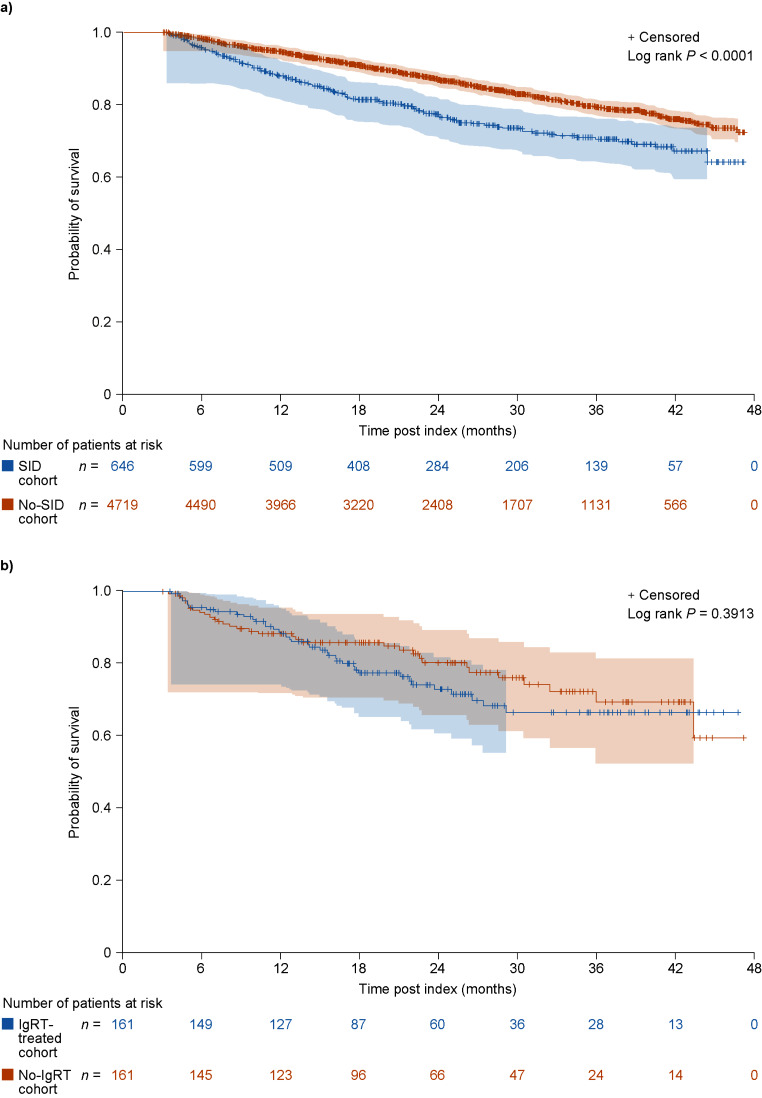
Patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and secondary immunodeficiency disease (SID) are susceptible to severe, recurrent, or persistent infections. This retrospective cohort study assessed the burden of infection in patients with CLL/SLL with and without SID, and in immunoglobulin replacement therapy (IgRT)-treated and -untreated patients with CLL/SLL and SID. Anonymized data from the US Optum-Humedica database (Oct-1-2015-Mar-10-2020) were used. Eligible patients aged ≥ 18 years with a confirmed CLL/SLL diagnosis were assigned to cohorts (SID or no-SID) using an algorithm based on serum IgG levels < 5.0 g/L, hypogammaglobulinemia diagnosis codes, and ≥ 1 major infection. A further sub-categorization was made based on patients with SID who received IgRT and those who did not. During 12-month follow-up, patients with CLL/SLL and SID were significantly more likely to experience infections (70.1% vs. 30.4%), including severe bacterial infections (39.8% vs. 9.2%), and infections requiring hospitalization (27.7% vs. 5.8%) than patients without SID. The use of anti-infectives and healthcare resource utilization (HCRU) was also higher in the SID cohort versus the no-SID cohort. Overall survival was shorter in patients with SID than those without (12.3 vs. 16.9 months). In patients with CLL/SLL and SID, burden of infection and HCRU were greater in IgRT-treated patients than in no-IgRT patients, potentially highlighting the IgRT-treated cohort as a more vulnerable population. Increasing understanding of SID burden may help to improve outcomes in patients with CLL/SLL. Further research is needed to develop guidance for IgRT use and to assess the benefits of IgRT in this vulnerable population.
Keywords: Burden of illness; Chronic lymphocytic leukemia; Quality of life; Small lymphocytic lymphoma.
© 2024. The Author(s).
Conflict of interest statement
CS, CA-S, MK, KR, and DS are employees of Takeda Development Center Americas, Inc. and are Takeda shareholders. JR has served on speakers bureaus for Bristol Myers Squibb and Janssen, and has received consulting fees and served on advisory boards for Adaptive Biotechnologies, AstraZeneca, Bristol Myers Squibb, Celgene, Janssen, Karyopharm Therapeutics, Oncopeptides, Sanofi, Secura Bio, Takeda, and X4 Pharmaceuticals. MSD has received grant support (paid to his institution) and consulting fees from Ascentage Pharma, AstraZeneca, Bristol Myers Squibb, Genentech, MEI Pharma, Secura Bio, and TG Therapeutics, and consulting fees from AbbVie, Adaptive Biotechnologies, AstraZeneca, BeiGene, BMS, Eli Lilly, Genentech, Genmab, Janssen, Merck, MingSight, Nuvalent, Secura Bio, Takeda, and TG Therapeutics.
Figures

References
-
- Jolles S, Giralt S, Kerre T, Lazarus HM, Mustafa SS, Papanicolaou GA et al (2023) Secondary antibody deficiency in chronic lymphocytic leukemia and non-hodgkin lymphoma: recommendations from an international expert panel. Blood Rev 58:101020. 10.1016/j.blre.2022.101020
-
- Kabadi SM, Near A, Wada K, Burudpakdee C (2020) Real-world treatment patterns, adverse events, resource use, and costs among commercially insured, younger patients with chronic lymphocytic leukemia in the USA: a retrospective cohort study. Adv Ther 37:3129–3148. 10.1007/s12325-020-01350-w - PubMed
-
- Freeman JA, Crassini KR, Best OG, Forsyth CJ, Mackinlay NJ, Han P et al (2013) Immunoglobulin G subclass deficiency and infection risk in 150 patients with chronic lymphocytic leukemia. Leuk Lymphoma 54:99–104. 10.3109/10428194.2012.706285 - PubMed
-
- Keegan A, Dennington PM, Dhondy N, Mulligan SP (2022) Immunoglobulin replacement therapy in chronic lymphocytic leukaemia patients with hypogammaglobulinaemia and infection. Eur J Haematol 108:460–468. 10.1111/ejh.13754 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
