

Idiopathic Distal Sensory Polyneuropathy and Fibromyalgia Syndrome: A Comparative Phenotyping Study
- PMID: 39264538
- PMCID: PMC11543958
- DOI: 10.1007/s40122-024-00646-x
Idiopathic Distal Sensory Polyneuropathy and Fibromyalgia Syndrome: A Comparative Phenotyping Study
Abstract
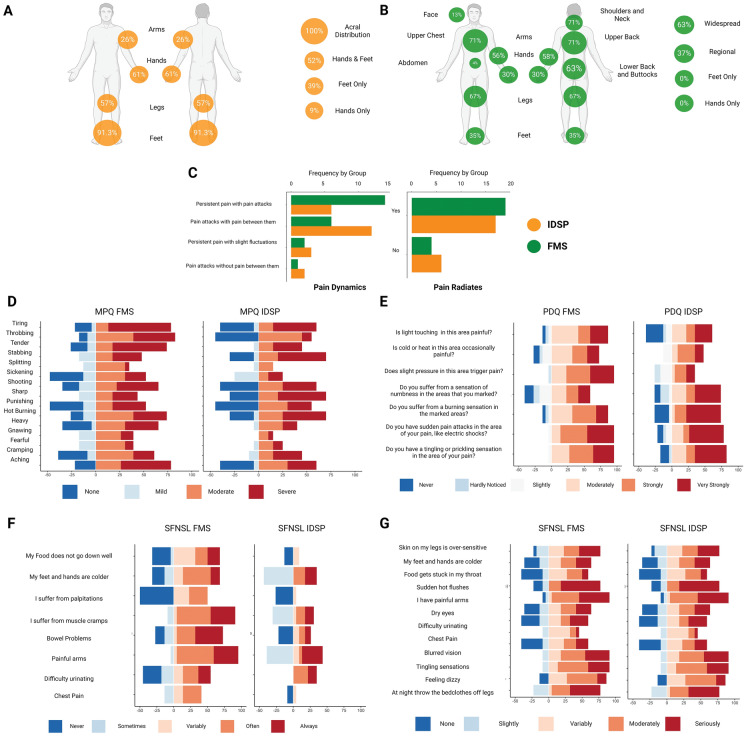
Introduction: Painful idiopathic distal sensory polyneuropathy (IDSP) and fibromyalgia syndrome (FMS) are cryptogenic chronic pain syndromes. The contribution of small fibre pathology (SFP) in FMS remains controversial. This study aims to quantify small nerve pathology in participants with IDSP and FMS and identify relationships of SFP with sensory phenotypes.
Methods: In this study, 73 individuals (FMS: 25, IDSP: 23, healthy volunteers: 25) underwent comprehensive assessment, including neurological exams, questionnaires, sensory tests, and corneal confocal microscopy.
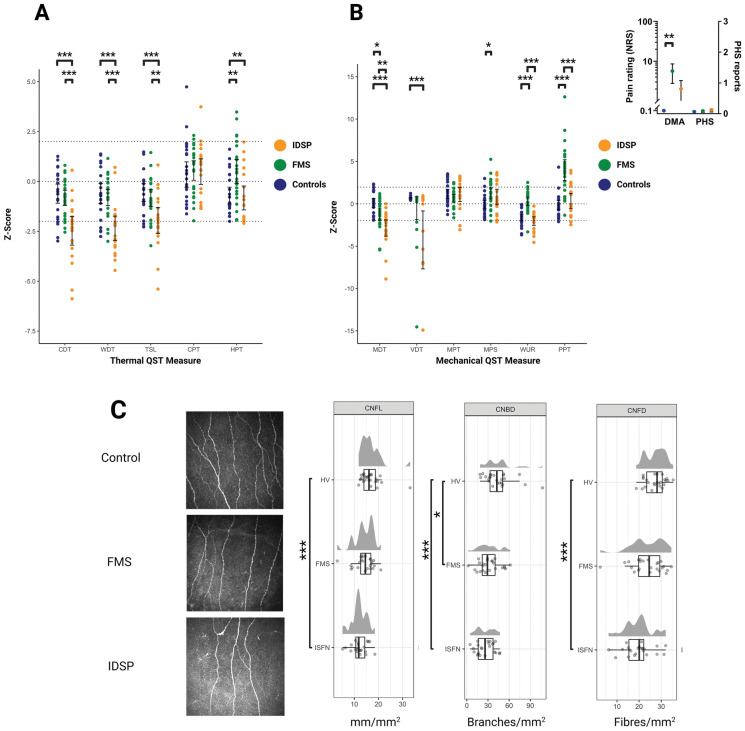
Results: IDSP participants displayed lower wind-up ratio (WUR) relative to FMS (p < 0.001), loss of function to thermal and mechanical stimuli and elevated neuropathy disability scores compared to FMS and healthy volunteers (all p < 0.001). FMS participants demonstrated gain of function to heat and blunt pressure pain responses relative to IDSP, and healthy volunteers (heat: p = 0.002 and p = 0.003; pressure: both p < 0.001) and WUR (both p < 0.001). FMS participants exhibited reduced corneal nerve fibre density (p = 0.02), while IDSP participants had lower global corneal nerve measures (density, branch density, and length) relative to healthy volunteers (all p < 0.001). Utilising corneal nerve fibre length, SFP was demonstrated in 66.6% of participants (FMS: 13/25; IDSP: 22/23).
Conclusion: Participants with SFP, in both FMS and IDSP, reported symptoms indicative of small nerve fibre disease. Although distinctions in pain distributions are evident between individuals with FMS and IDSP, over 50% of participants between the two conditions displayed both a loss and gain of thermal and mechanical function suggestive of shared mechanisms. However, sensory phenotypes were associated with the presence of SFP in IDSP but not in FMS.
Keywords: Corneal confocal microscopy; Fibromyalgia syndrome; Idiopathic distal sensory polyneuropathy; Neuropathic pain; Pain characteristics; Quantitative sensory testing; Sensory phenotyping; Small fibre.
Plain language summary
In people with painful idiopathic neuropathy (pain related to nerve damage where the cause of nerve damage is unknown), fibromyalgia syndrome (a long-term condition causing widespread pain), and healthy volunteers, the small nerve fibres of the peripheral nervous system, which may be involved in generating pain were assessed. These nerve fibres can be measured at the front of the eye (cornea) which can provide details on whether they are damaged in the body. The response to temperature, light touch, pressure and pinprick stimuli can also be used to determine if there is a loss or gain of sensation, which may contribute to pain. The aim of this study was to identify the degree of damage to these nerve fibres and to determine whether this damage is associated with a loss (cannot feel or requires more intense stimulus to feel) or gain (stimulus is felt earlier or is painful earlier at lower intensity) of sensory function. The pattern of loss or gain in sensory function is known as a sensory phenotype. It was found that people with painful idiopathic neuropathy had more severe nerve damage, loss of function to temperature and touch, and fewer small nerve fibres in the cornea compared to those with fibromyalgia syndrome and healthy volunteers. People with fibromyalgia syndrome were more sensitive to heat and pressure and had fewer corneal nerve fibres relative to healthy volunteers. The presence of corneal nerve fibre damage was associated with sensory phenotypes (types of sensation felt) in painful idiopathic neuropathy but not in fibromyalgia syndrome.
© 2024. The Author(s).
Conflict of interest statement
All authors; Jamie Burgess, Anne Marshall, Leandros Rapteas, David Riley, Kohei Matsumoto, Cheng Boon, Alia Alchawaf, Maryam Ferdousi, Rayaz A. Malik, Andrew Marshall, Stephen Kaye, David Gosal and Bernhard Frank declare that they have no competing interests relevant to the current publication. Uazman Alam has no direct conflict of interest but discloses the following: honoraria received from Procter & Gamble, Viatris, Eli Lilly, Grunenthal, and Sanofi for educational meetings; investigator-led funding from Procter & Gamble; and sponsorship for travel to an international conference from Daiichi Sankyo.
Figures
References
-
- Freeman R, Gewandter JS, Faber CG, Gibbons C, Haroutounian S, Lauria G, Levine T, Malik RA, Singleton JR, Smith AG, Bell J, Dworkin RH, Feldman E, Herrmann DN, Hoke A, Kolb N, Mansikka H, Oaklander AL, Peltier A, Polydefkis M, Ritt E, Russell JW, Sainati S, Steiner D, Treister R, Üçeyler N. Idiopathic distal sensory polyneuropathy. Neurology. 2020;95(22):1005. - DOI - PMC - PubMed
-
- Häuser W, Brähler E, Ablin J, Wolfe F. Modified 2016 American College of Rheumatology Fibromyalgia Criteria, the Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks-American Pain Society Pain Taxonomy, and the prevalence of fibromyalgia. Arthritis Care Res (Hoboken). 2021;73(5):617–25. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
