

Outcomes with single-agent gilteritinib for relapsed or refractory FLT3-mutant AML after contemporary induction therapy
- PMID: 39265176
- PMCID: PMC11541456
- DOI: 10.1182/bloodadvances.2024014017
Outcomes with single-agent gilteritinib for relapsed or refractory FLT3-mutant AML after contemporary induction therapy
Abstract
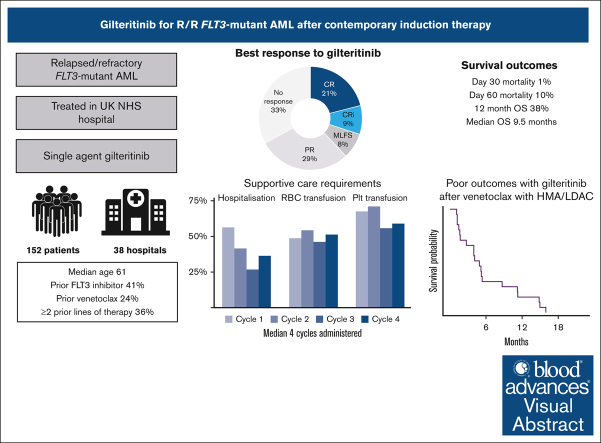
Gilteritinib is the current standard of care for relapsed or refractory fms related receptor tyrosine kinase 3 (FLT3)-mutated acute myeloid leukemia in many countries, however outcomes for patients relapsing after contemporary first-line therapies (intensive chemotherapy with midostaurin, or nonintensive chemotherapy with venetoclax) are uncertain. Moreover, reported data on toxicity and health care resource use is limited. Here, we describe a large real-world cohort of 152 patients receiving single-agent gilteritinib in 38 UK hospitals. Median age was 61 years, and 36% had received ≥2 prior lines of therapy, including a FLT3 inhibitor in 41% and venetoclax in 24%. A median of 4 cycles of gilteritinib were administered, with 56% of patients requiring hospitalization in the first cycle (median, 10 days). Over half of patients required transfusion in each of the first 4 cycles. Complete remission (CR) was achieved in 21%, and CR with incomplete recovery (CRi) in a further 9%. Remission rates were lower for patients with FLT3-tyrosine kinase domain or adverse karyotype. Day-30 and day-60 mortality were 1% and 10.6%, respectively, and median overall survival was 9.5 months. On multivariable analysis, increasing age, KMT2A rearrangement, and complex karyotype were associated with worse survival whereas RUNX1 mutations were associated with improved survival. Twenty patients received gilteritinib as first salvage having progressed after first-line therapy with venetoclax, with CR/CRi achieved in 25% and median survival 4.5 months. Real-world results with gilteritinib mirror those seen in the clinical trials, but outcomes remain suboptimal, with more effective strategies needed.
© 2024 by The American Society of Hematology. This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
Conflict-of-interest disclosure: J. Othman declares honoraria from Astellas and Jazz Pharmaceuticals. A.H. declares honoraria from Kite/Gilead. P.G. declares honoraria from Astellas. R. Dang declares meeting sponsorship from Jazz; and honoraria from AbbVie. J.V. declares meeting support from BeiGene, Janssen, and Jazz; and reports honoraria from AbbVie and AstraZeneca. P.K. declares honoraria from Jazz, Astellas, and Gilead; reports speakers bureau role with Astellas; and reports consultancy for Jazz and Gilead. A.-L.L. declares honoraria from Astella, AbbVie, Amgen, Kite, Novartis, Jazz, and Daiichi Sankyo; and speakers bureau role with Kite, Takeda, and Astellas. F.H. declares meeting sponsorship and honoraria from AbbVie. J.L. declares honoraria from Aptitude health. N.F. declares investigator meetings with Novartis and MEI Pharma. J. O’nions declares honoraria from Servier, Astellas, AbbVie, Jazz, and Janssen. Anjum Khan declares meeting sponsorship from Jazz, Medac, and Servier; speakers bureau role with AbbVie, Astellas, Jazz, and Servier; and consultancy/advisory board role for TC BioPharm, Incyte, Immedica, Novartis, Synairgen, and Takeda. R. Dillon declares research funding from AbbVie and Amgen; and consultancy with Astellas, Pfizer, Novartis, Jazz, BeiGene, Shattuck, and AvenCell. The remaining authors declare no competing financial interests.
Figures


References
-
- Thiede C, Steudel C, Mohr B, et al. Analysis of FLT3-activating mutations in 979 patients with acute myelogenous leukemia: association with FAB subtypes and identification of subgroups with poor prognosis. Blood. 2002;99(12):4326–4335. - PubMed
-
- Kottaridis PD, Gale RE, Frew ME, et al. The presence of a FLT3 internal tandem duplication in patients with acute myeloid leukemia (AML) adds important prognostic information to cytogenetic risk group and response to the first cycle of chemotherapy: analysis of 854 patients from the United Kingdom Medical Research Council AML 10 and 12 trials. Blood. 2001;98(6):1752–1759. - PubMed
-
- Mead AJ, Linch DC, Hills RK, Wheatley K, Burnett AK, Gale RE. FLT3 tyrosine kinase domain mutations are biologically distinct from and have a significantly more favorable prognosis than FLT3 internal tandem duplications in patients with acute myeloid leukemia. Blood. 2007;110(4):1262–1270. - PubMed
-
- Gale RE, Green C, Allen C, et al. The impact of FLT3 internal tandem duplication mutant level, number, size, and interaction with NPM1 mutations in a large cohort of young adult patients with acute myeloid leukemia. Blood. 2008;111(5):2776–2784. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
