

Multinational trends in sepsis mortality between 1985 and 2019: a temporal analysis of the WHO Mortality Database
- PMID: 39266316
- PMCID: PMC11404178
- DOI: 10.1136/bmjopen-2023-074822
Multinational trends in sepsis mortality between 1985 and 2019: a temporal analysis of the WHO Mortality Database
Abstract
Objectives: Understanding the burden of disease of sepsis is essential for monitoring the effectiveness of international strategies to improve sepsis care. Our objective was to describe the multinational trend of sepsis-related mortality for the period 1985-2019 from the WHO Mortality Database.
Design: Retrospective analysis of the WHO Mortality Database.
Setting: We included data from all countries defined by the WHO as having 'high usability data' and at least 10 years of total available data.
Participants: From the WHO list of 50 countries with high usability data, 14 (28%) were excluded due to excessive missingness. We included and analysed data separately for male and female.
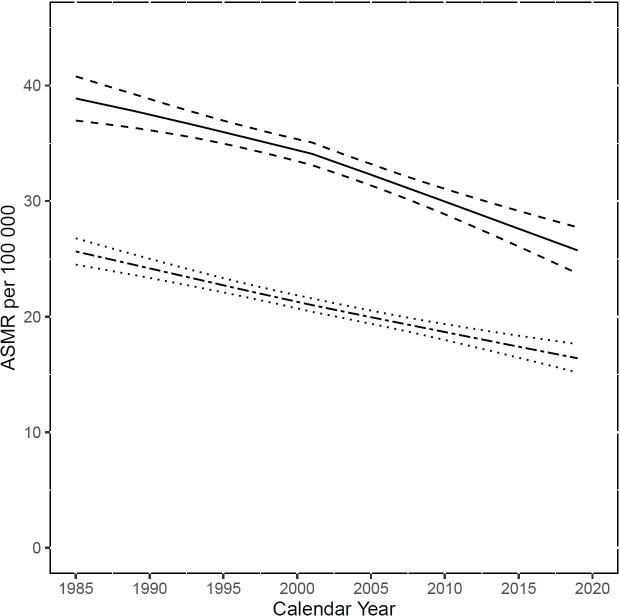
Primary and secondary outcome measures: We analysed age-standardised mortality rates (ASMR) (weighted average of the age-specific mortality rates per 100 000 people, where the weights are the proportions of people in the corresponding age groups of the WHO standard population).
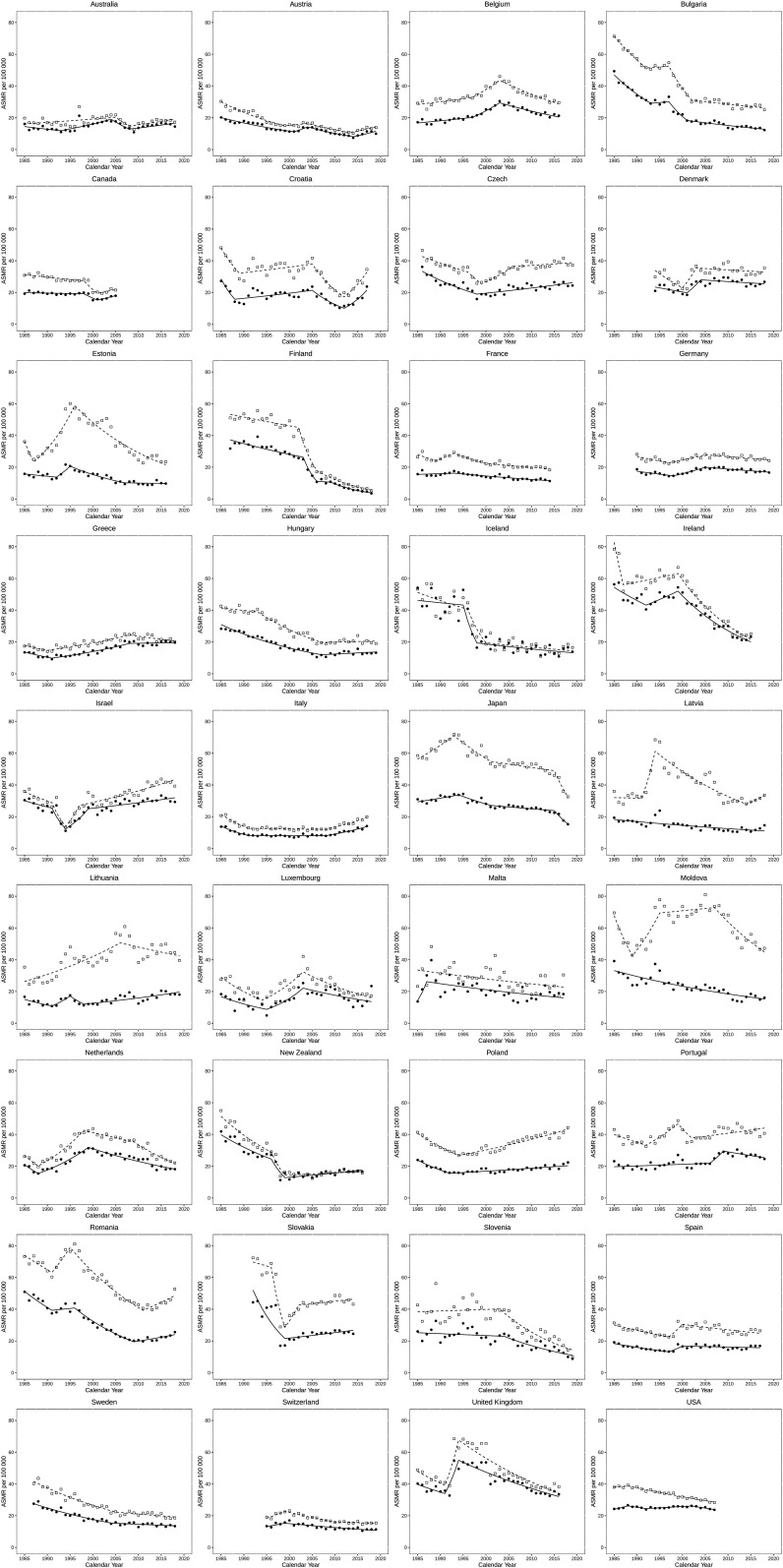
Results: We included 1104 country-years worth of data from 36 countries with high usability data, accounting for around 15% of the world's population. The median ASMR for men decreased from 37.8 deaths/100 000 (IQR 28.4-46.7) in 1985-1987 to 25.8 deaths/100 000 (IQR 19.2-37) in 2017-2019, an approximately 12% absolute (31.8% relative) decrease. For women, the overall ASMR decreased from 22.9 deaths/100 000 (IQR 17.7-32.2) to 16.2 deaths/100 000 (IQR 12.6-21.6), an approximately 6.7% absolute decrease (29.3% relative decrease). The analysis of country-level data revealed wide variations in estimates and trends.
Conclusions: We observed a decrease in reported sepsis-related mortality across the majority of analysed nations between 1985 and 2019. However, significant variability remains between gender and health systems. System-level and population-level factors may contribute to these differences, and additional investigations are necessary to further explain these trends.
Keywords: epidemiology; infectious diseases; intensive & critical care.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Torio CM, Andrews RM. Healthcare Cost and Utilization Project (HCUP) statistical briefs. Rockville, MD: Agency for Health Care Policy and Research (US); 2013. National inpatient hospital costs: the most expensive conditions by payer, 2011: statistical brief #160. - PubMed
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–55. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical