

Effect of hearing intervention on communicative function: A secondary analysis of the ACHIEVE randomized controlled trial
- PMID: 39266468
- PMCID: PMC11637286
- DOI: 10.1111/jgs.19185
Effect of hearing intervention on communicative function: A secondary analysis of the ACHIEVE randomized controlled trial
Abstract
Background: The Aging and Cognitive Health Evaluation in Elders (ACHIEVE) Study was designed to determine the effects of a best-practice hearing intervention on cognitive decline among community-dwelling older adults. Here, we conducted a secondary analysis of the ACHIEVE Study to investigate the effect of hearing intervention on self-reported communicative function.
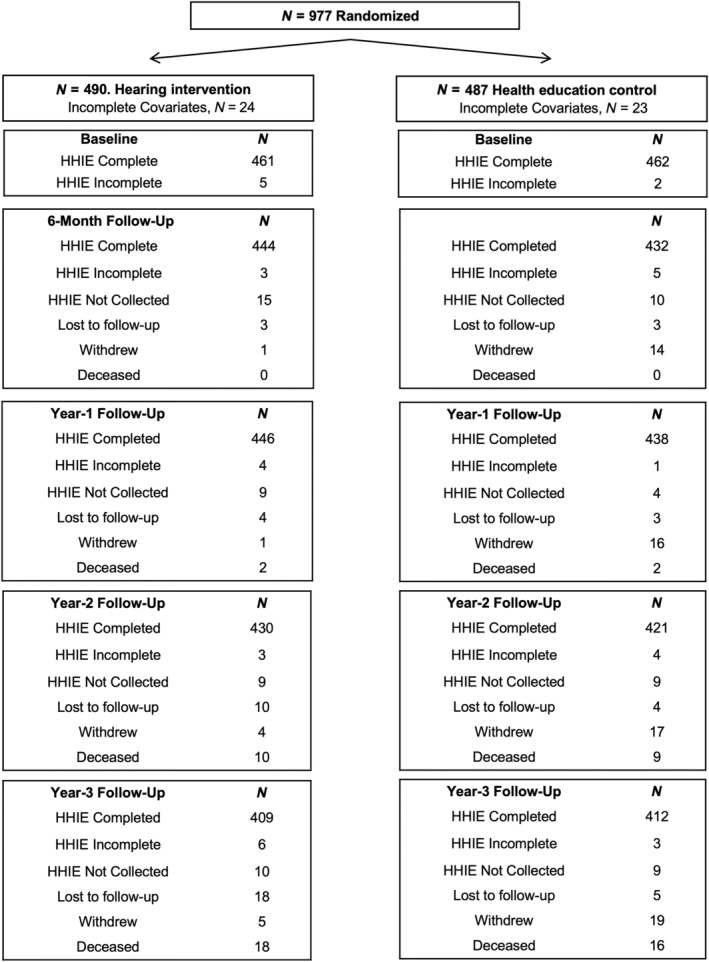
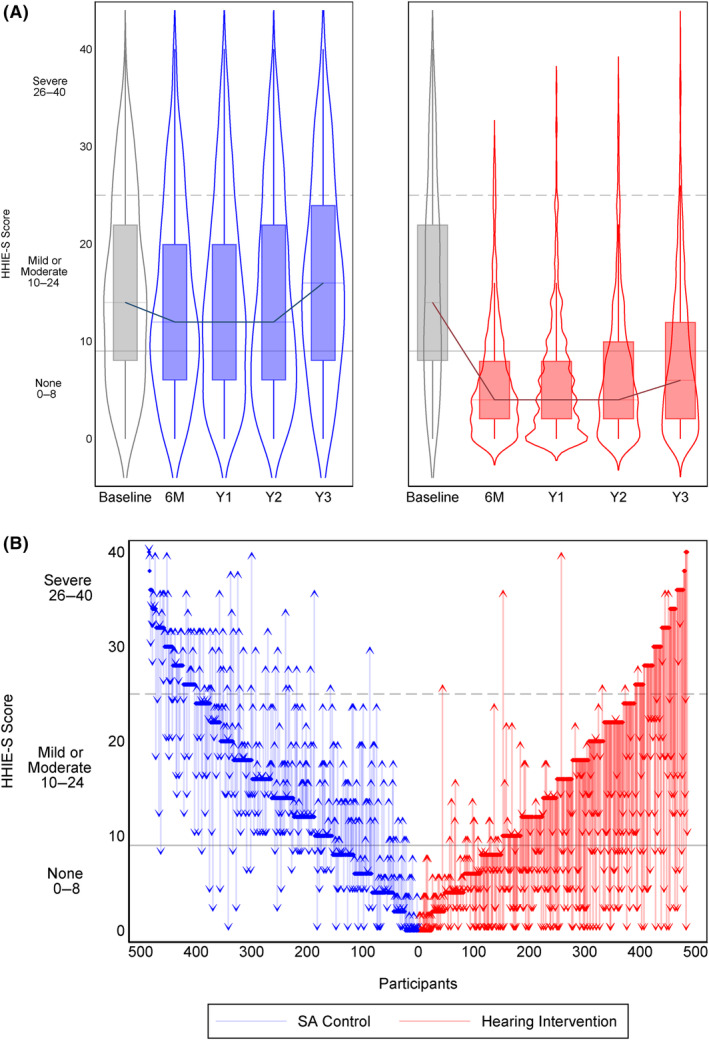
Methods: The ACHIEVE Study is a parallel-group, unmasked, randomized controlled trial of adults aged 70-84 years with untreated mild-to-moderate hearing loss and without substantial cognitive impairment. Participants were randomly assigned (1:1) to a hearing intervention (audiological counseling and provision of hearing aids) or a control intervention of health education (individual sessions with a health educator covering topics on chronic disease prevention) and followed semiannually for 3 years. Self-reported communicative function was measured with the Hearing Handicap Inventory-Elderly Screening version (HHIE-S, range 0-40, higher scores indicate greater impairment). Effect of hearing intervention versus control on HHIE-S was analyzed through an intention-to-treat model controlling for known covariates.
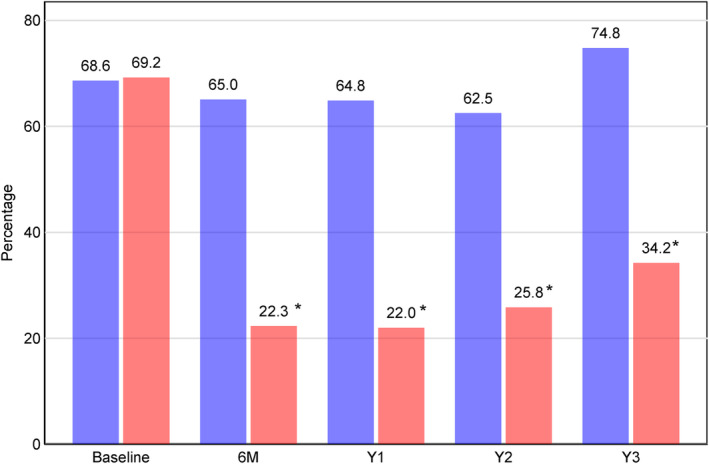
Results: HHIE-S improved after 6-months with hearing intervention compared to control, and continued to be better through 3-year follow-up. We estimated a difference of -8.9 (95% CI: -10.4, -7.5) points between intervention and control groups in change in HHIE-S score from baseline to 6 months, -9.3 (95% CI: -10.8, -7.9) to Year 1, -8.4 (95% CI: -9.8, -6.9) to Year 2, and - 9.5 (95% CI: -11.0, -8.0) to Year 3. Other prespecified sensitivity analyses that varied analytical parameters did not change the observed results.
Conclusions: Hearing intervention improved self-reported communicative function compared to a control intervention within 6 months and with effects sustained through 3 years. These findings suggest that clinical recommendations for older adults with hearing loss should encourage hearing intervention that could benefit communicative function and potentially have positive downstream effects on other aspects of health.
Keywords: clinical trial; cognition; functional disability; hearing handicap; hearing loss.
© 2024 The Author(s). Journal of the American Geriatrics Society published by Wiley Periodicals LLC on behalf of The American Geriatrics Society.
Conflict of interest statement
Dr. Sanchez reported industry funding related to consulting or research support from Otonomy Inc., Autifony Therapeutics Ltd., Boehringer Ingelheim, Frequency Therapeutics Ltd., Pipeline Therapeutics, Aerin Medical, Oticon Medical, Helen of Troy Ltd., Sonova Holding AG, and Phonak USA. Dr. Reed reported serving on the scientific advisory boards of Neosensory. Dr. Schrack is a consultant to Edwards Lifesciences. Dr. Lin reported being a consultant to Frequency Therapeutics and Apple and being the director of a research center funded in part by a philanthropic gift from Cochlear Ltd to the Johns Hopkins Bloomberg School of Public Health. Dr. Lin is also a board member of the nonprofit Access HEARS. All other authors report no relevant disclosures.
Figures
References
-
- National Academies of Sciences Engineering and Medicine . Hearing Health Care for Adults: Priorities for Improving Access and Affordability. The National Academies Press; 2016. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- 2U01HL096917/NH/NIH HHS/United States
- R01AG060502/AG/NIA NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- NIAR34AG046548/AG/NIA NIH HHS/United States
- R01 AG055426/AG/NIA NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- 2U01HL096814/NH/NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- R01AG055426/AG/NIA NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- U01 2U01HL096812/NH/NIH HHS/United States
- R01 AG060502/AG/NIA NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- R34 AG046548/AG/NIA NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- Eleanor Schwartz Charitable Foundation
- R01 AG076518/AG/NIA NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- 2U01HL096899/NH/NIH HHS/United States
- R01 DC019408/DC/NIDCD NIH HHS/United States
- Sonova/Phonak LLC
- 2U01HL096902/NH/NIH HHS/United States
- R01HL70825/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
