

Trends and determinants of the use of episiotomy in a prospective population-based registry from central India
- PMID: 39267006
- PMCID: PMC11396254
- DOI: 10.1186/s12884-024-06762-y
Trends and determinants of the use of episiotomy in a prospective population-based registry from central India
Abstract
Background: Findings from research and recommendations from the World Health Organization favor restrictive use of episiotomy, but whether this guidance is being followed in India, and factors associated with its use, are not known. This study sought to document trends in use of episiotomy over a five-year period (2014-2018); to examine its relationship to maternal, pregnancy, and health-system characteristics; and to investigate its association with other obstetric interventions.
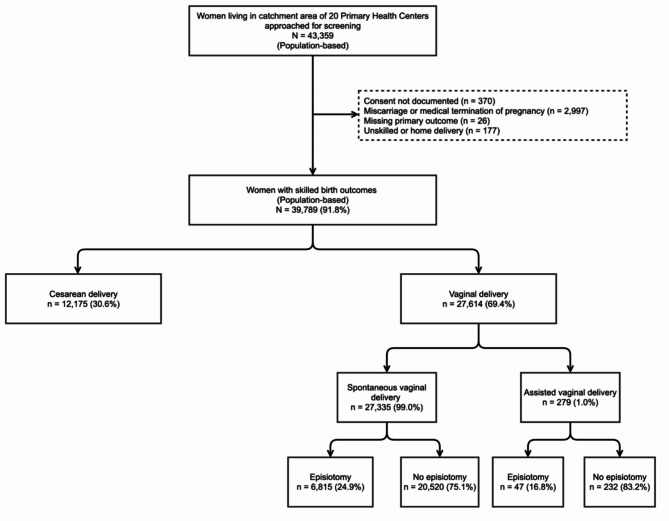
Methods: We conducted a secondary analysis of data collected by the Maternal Newborn Health Registry, a prospective population-based pregnancy registry established in Central India (Nagpur, Eastern Maharashtra). We examined type of birth and use of episiotomy in vaginal deliveries from 2014 to 2018, as well as maternal and birth characteristics, health systems factors, and concurrent obstetric interventions associations with its use with multivariable Poisson regression models.
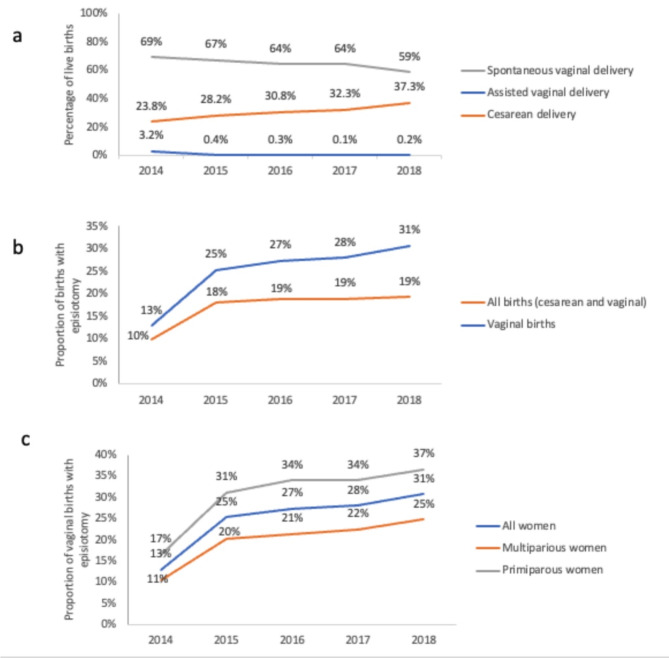
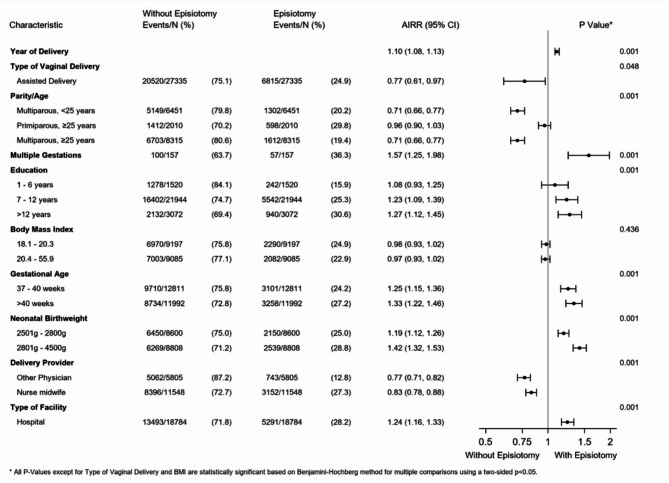
Results: During the five-year interval, the rate of episiotomy in vaginal birth rose from 13 to 31% despite a decline in assisted vaginal birth. Associations with episiotomy were found for the following factors: prior birth, multiple gestations, seven or more years of maternal education, higher gestational age, higher birthweight, delivery by an obstetrician (as compared to midwife or general physician), and birth in hospital (as compared to clinic or health center). After adjusting for these factors, year over year rise in episiotomy was significant with an adjusted incidence rate ratio (AIRR) of 1.10 [95% confidence interval (CI) 1.08-1.12; p = 0.002]. We found an association between episiotomy and several other obstetric interventions, with the strongest relationship for maternal treatment with antibiotics (AIRR 4.23, 95% CI 3.12-5.73; p = 0.001).
Conclusions: Episiotomy in this population-based sample from central India steadily rose from 2014 to 2018. This increase over time was observed even after adjusting for patient characteristics, obstetric risk factors, and health system features, such as specialty of the birthing provider. Our findings have important implications for maternal-child health and respectful maternity care given that most women prefer to avoid episiotomy; they also highlight a potential target for antibiotic stewardship as part of global efforts to combat antimicrobial resistance.
Trial registration: The study was registered at ClinicalTrials.gov under reference number NCT01073475.
Keywords: Birth complications; Episiotomy; India; Vaginal birth.
Plain language summary
Episiotomy is a surgical procedure to widen the vaginal opening for childbirth. It was once commonly used worldwide. However, because the procedure can cause pain to mothers and place them at risk for infections and serious tears to the vagina—especially when the cut is directly downward—research suggests it should be used sparingly. As such, it is now less often practiced in high-income countries, but whether the same is true in India is not known. To answer this question, we used a large population-based pregnancy registry, the Maternal Newborn Health Registry, from Central India (Nagpur) to assess the frequency of episiotomy use between 2014 and 2018 and if there were certain maternal characteristics, features of the health care system, and other pregnancy interventions that were related with its use. Over this five-year period, the use of episiotomy during vaginal birth rose more than two-fold. It was more often used on women who had never delivered a baby before, were further along in pregnancy, had higher levels of education, had heavier babies, or were carrying more than one baby. Obstetricians were more likely to perform episiotomy than midwives or general physicians and it was more likely to be performed in hospitals than in clinics or primary health centers. This rise during the five-year interval was significant even when accounting for these patient and provider characteristics, suggesting a shift in medical practice. Because this was an observational study more research is needed to determine if the associations we found are causal.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Thacker SB, Banta HD. Benefits and risks of episiotomy: an interpretative review of the English language literature, 1860–1980. Vol. 38, Obstetrical & gynecological survey. Baltimore:; 1983. pp. 322–38. - PubMed
-
- Harrison MS, Ali S, Pasha O, Saleem S, Althabe F, Berrueta M, et al. A prospective population-based study of maternal, fetal, and neonatal outcomes in the setting of prolonged labor, obstructed labor and failure to progress in low- and middle-income countries. Reprod Health. 2015;12(Suppl 2):S9. 10.1186/1742-4755-12-S2-S9 - DOI - PMC - PubMed
-
- Berkowitz L, Foust-Wright C, UpToDate. Waltham MA, Editors CJ, Lockwood K, Eckler, editors. ; 2020 [cited 2021 Oct 12]. Approach to episiotomy. https://www.uptodate.com/contents/approach-to-episiotomy?search=episioto...
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
