

Meta-analysis of bone mineral density in adults with phenylketonuria
- PMID: 39267130
- PMCID: PMC11391789
- DOI: 10.1186/s13023-024-03223-9
Meta-analysis of bone mineral density in adults with phenylketonuria
Abstract
Background: Lifelong management of phenylketonuria (PKU) centers on medical nutrition therapy, including dietary phenylalanine (Phe) restriction in addition to Phe-free or low-Phe medical foods/protein substitutes. Studies have reported low bone mineral density (BMD) in mixed-age PKU populations, possibly related to long-term Phe restriction. Therefore, a meta-analysis investigating BMD specifically in adults with PKU was conducted.
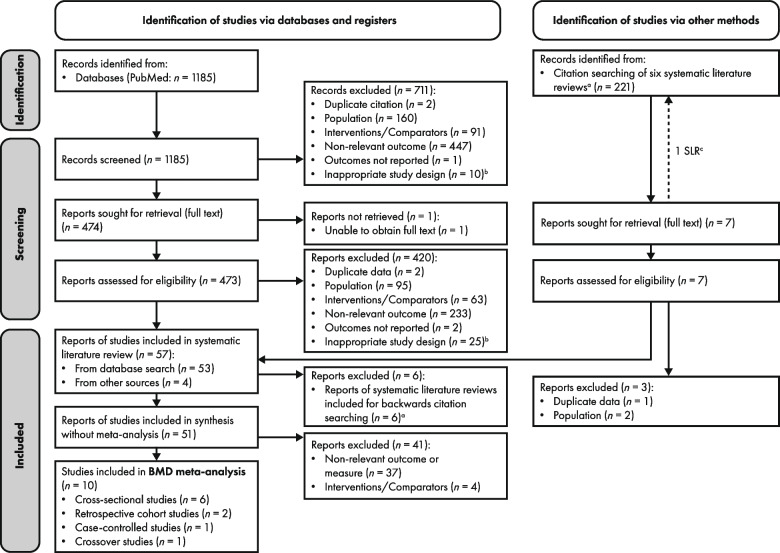
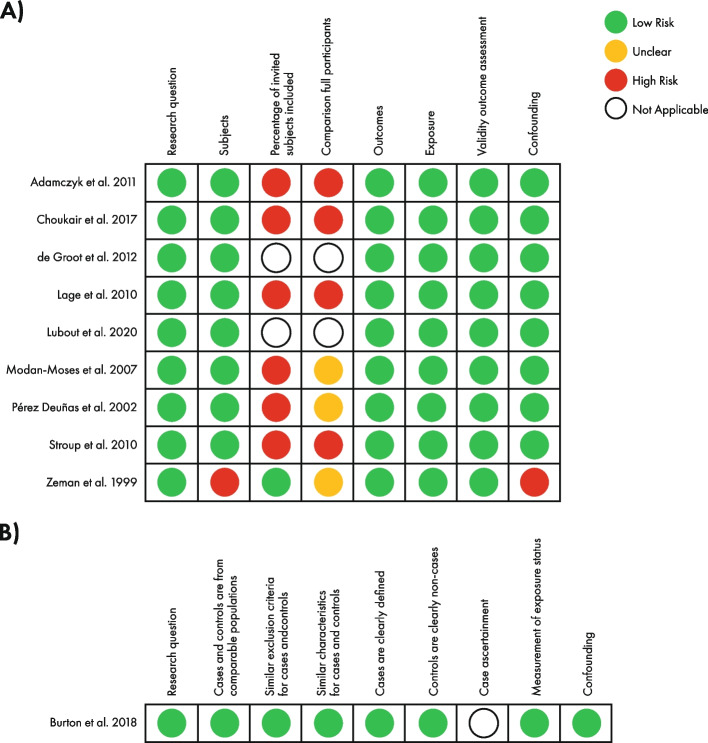
Methods: Studies reporting BMD-related outcomes were identified from a systematic literature review evaluating somatic comorbidities experienced by adults with PKU on a Phe-restricted diet (searched February 1, 2022, updated November 1, 2023). Risk of study bias was assessed (Scottish Intercollegiate Guidelines Network checklists). The primary outcome of the meta-analysis was pooled mean BMD Z-scores of different bones. Secondary outcomes were the prevalence of low BMD Z-scores at pre-specified thresholds. Subgroup analyses of mean BMD Z-scores (decade of study publication, controlled versus uncontrolled blood Phe levels, gender) were conducted.
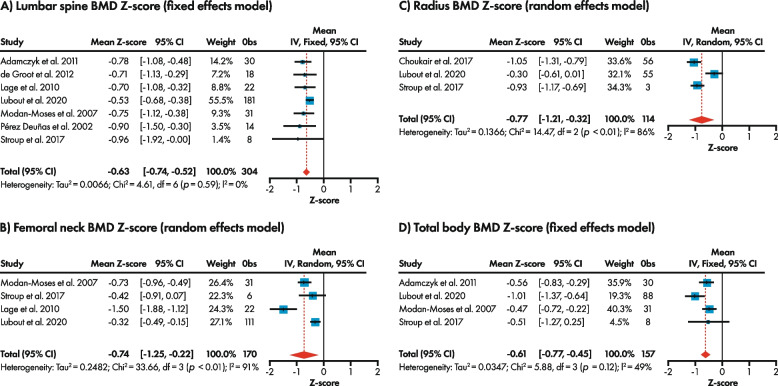
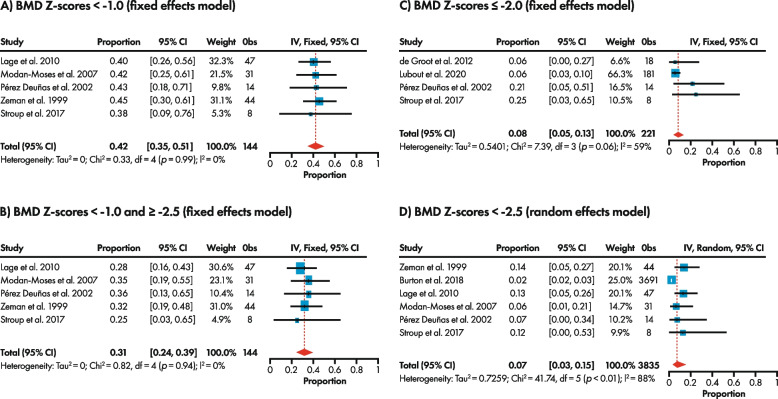
Results: BMD-related data from 4097 individuals across 10 studies rated as at least acceptable quality were included. Mean BMD Z-scores were statistically significantly lower compared with an age-matched control or reference (non-PKU) population, across bones, but still within the expected range for age (> -2.0): lumbar spine (seven studies, n = 304), -0.63 (95% confidence interval (CI): -0.74, -0.52); femoral neck (four studies, n = 170), -0.74 (95% CI: -1.25, -0.22); radius (three studies, n = 114), -0.77 (95% CI: -1.21, -0.32); total body (four studies, n = 157), -0.61 (95% CI: -0.77, -0.45). The small number of observations in the subgroup analyses resulted in a high degree of uncertainty, limiting interpretation. Estimated prevalence of BMD Z-scores ≤ -2.0 was 8% (95% CI: 5%, 13%; four studies, n = 221) and < -1.0 was 42% (95% CI: 35%, 51%; five studies, n = 144).
Conclusions: Adults with PKU had lower BMD Z-scores than the reference (non-PKU) population but < 1 in 10 were below the expected range for age. The low number of studies prevents identification of which population characteristics are most impacting BMD. This meta-analysis was supported by BioMarin Pharmaceutical Inc., Novato, CA and is registered with the Research Registry (reviewregistry1476).
Keywords: Bone; Bone mineral density; Diet; Diet adherence; Meta-analysis; Osteopenia; Osteoporosis; Phenylalanine; Phenylketonuria; Z-score.
© 2024. The Author(s).
Conflict of interest statement
JCR has received consulting payments from Applied Pharma Research, BioMarin, Merck Serono, Nutricia, PTC Therapeutics, and Synlogic Therapeutics; speaker fees/payments from Applied Pharma Research, BioMarin, Cambrooke, LifeDiet, Merck Serono, Nutricia, PIAM, and Vitaflo; travel support from Applied Pharma Research, BioMarin, Glutamine, Merck Serono, PIAM; and research grants from BioMarin. AH has received consulting payments from Amicus Therapeutics, BioMarin, Chiesi, Genzyme, Shire, and Ultragenyx; speaker fees/payments from Alexion, Amicus Therapeutics, BioMarin, Genzyme, InMedica, Nutricia, Sobi, Takeda, and Vitaflo; travel support from Amicus Therapeutics, BioMarin, Chiesi, Genzyme, Inmedica, Sobi, and Vitaflo; and has participated as a clinical trial investigator for Ultragenyx. At the time this work was undertaken, CJJ and YW were employees of HCD Economics, a company sponsored by BioMarin to conduct this study and prepare the manuscript. GEC, SR, and KBW are employees and stockholders of BioMarin. KKA has received consulting payments from Arla Foods Ingredients, BioMarin, Homology, and Nutricia. ALSP has received speaker fees/payments from BioMarin. COH has received consulting and speaker fees/payments from BioMarin and has participated as a clinical trial investigator for BioMarin. FR is a managing partner of Met Ed who has received educational grants from BioMarin. AI has received consulting payments for and travel support to advisory boards from BioMarin. NL has received consulting payments for advisory boards from Alnylam, Amicus Therapeutics, Audentes/Astellas, BioMarin, BridgeBio/CoA Therapeutics, Chiesi/Protalix, Genzyme/Sanofi, HemoShear Therapeutics, Horizon Pharma, Jaguar Gene Therapy, Jnana Therapeutics, Leadiant Biosciences, Moderna, Nestlé Pharma, PTC Therapeutics, Recordati, Reneo, Takeda, and Ultragenyx; has received other consultancy payments from Synlogic Therapeutics; has received travel support from BioMarin; has participated as a clinical trial investigator for Aeglea, Amicus Therapeutics, Audentes/Astellas, AVROBIO, BioMarin, Chiesi/Protalix, Genzyme/Sanofi, HemoShear Therapeutics, Homology, Horizon Pharma, Moderna, Nestlé Pharma, Pfizer, PTC Therapeutics, Reneo, Synlogic Therapeutics, Takeda, Travere Therapeutics, and Ultragenyx; and has been Data Safety and Monitoring Chair for ACI Clinical. ACM has received consulting payments from Atheneum, Nestlé, and PTC Therapeutics; speaker fees/payments from AIM, Applied Pharma Research, and Nutricia; travel support from Nutricia; and has participated as a clinical trial investigator for Nutricia. SS has received speaker fees/payments from BioMarin and Sanofi. FM has received consulting payments from PTC Therapeutics and travel support from BioMarin.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
