

Machine learning models from computed tomography to diagnose thymic epithelial tumors requiring combined resection
- PMID: 39268145
- PMCID: PMC11388251
- DOI: 10.21037/jtd-23-1840
Machine learning models from computed tomography to diagnose thymic epithelial tumors requiring combined resection
Abstract
Background: Minimally invasive approaches have been a standard choice of surgery for noninvasive thymic epithelial tumors (TETs), but we sometimes experience cases requiring combined resection of adjacent structures. We develop and validate machine learning models to predict combined resection based on preoperative contrast-enhanced computed tomography (CT).
Methods: This study included 212 patients with TETs (140 in the training cohort and 72 in the validation cohort) who underwent radical surgery. Radiomics features were extracted from contrast-enhanced CT and predicted with five feature selection methods and seven machine learning models in nested cross validation. The clinical utility of the models was analyzed by a decision curve analysis (DCA).
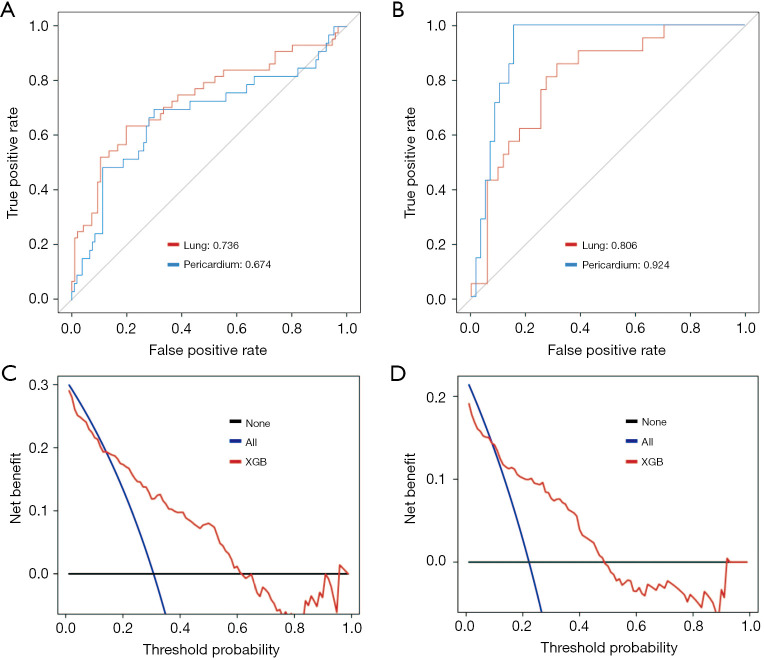
Results: Fifty-five patients in the training cohort and 28 in the validation cohort required combined resection. The classifiers random forest (RF), gradient boosting (GB), and eXtreme Gradient Boosting (XGB) indicated high predictive performance, with the XGB classifier based on features selected by GB performing the best, with an area under the curve (AUC) of 0.797. In the validation cohort, the classifier had an AUC of 0.817. The DCA showed the validity of the model with a threshold range of 15-72%. When restricted to combined pulmonary and pericardial resection, the respective AUCs were 0.736 and 0.674 for the training cohort and 0.806 and 0.924 for the validation cohort.
Conclusions: The machine learning model based on preoperative CT images was able to diagnose TETs requiring combined resection with high accuracy. The DCA demonstrated a wide range of model validity and may aid in surgical approach selection.
Keywords: Thymic epithelial tumor (TET); computed tomography (CT); machine learning; radiomics; surgical procedure.
2024 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-1840/coif). I.Y. receives grants from Taiho Pharmaceutical, Chugai Pharmaceutical, Shionogi Pharmaceutical, Daiichi-sankyo Chemial Pharma, Eli Lily and Pfizer; consulting fees from Astra Zeneca, Chugai Pharmaceutical, Johnson and Johnson, Medicaroid, Covidien and Intuitive Surgical; honoraria from Astra Zeneca, Chugai Pharmaceutical, Johnson and Johnson, Covidien Japan, Daiichi-sankyo Chemical Pharma, Taho, Eli Lily, Intuitive Surgical, MSD and Bristol-Myers Squib. The other authors have no conflicts of interest to declare.
Figures



References
-
- Committee for Scientific Affairs , The Japanese Association for Thoracic Surgery, Shimizu H, et al. Thoracic and cardiovascular surgeries in Japan during 2018 : Annual report by the Japanese Association for Thoracic Surgery. Gen Thorac Cardiovasc Surg 2021;69:179-212. 10.1007/s11748-020-01460-w - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources