

Utility of Skin Tone on Pulse Oximetry in Critically Ill Patients: A Prospective Cohort Study
- PMID: 39268149
- PMCID: PMC11392475
- DOI: 10.1097/CCE.0000000000001133
Utility of Skin Tone on Pulse Oximetry in Critically Ill Patients: A Prospective Cohort Study
Abstract
Objective: Pulse oximetry, a ubiquitous vital sign in modern medicine, has inequitable accuracy that disproportionately affects minority Black and Hispanic patients, with associated increases in mortality, organ dysfunction, and oxygen therapy. Previous retrospective studies used self-reported race or ethnicity as a surrogate for skin tone which is believed to be the root cause of the disparity. Our objective was to determine the utility of skin tone in explaining pulse oximetry discrepancies.
Design: Prospective cohort study.
Setting: Patients were eligible if they had pulse oximetry recorded up to 5 minutes before arterial blood gas (ABG) measurements. Skin tone was measured using administered visual scales, reflectance colorimetry, and reflectance spectrophotometry.
Participants: Admitted hospital patients at Duke University Hospital.
Interventions: None.
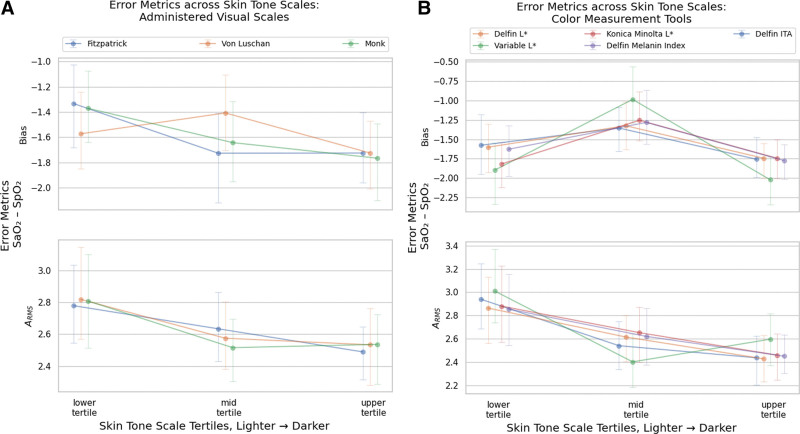
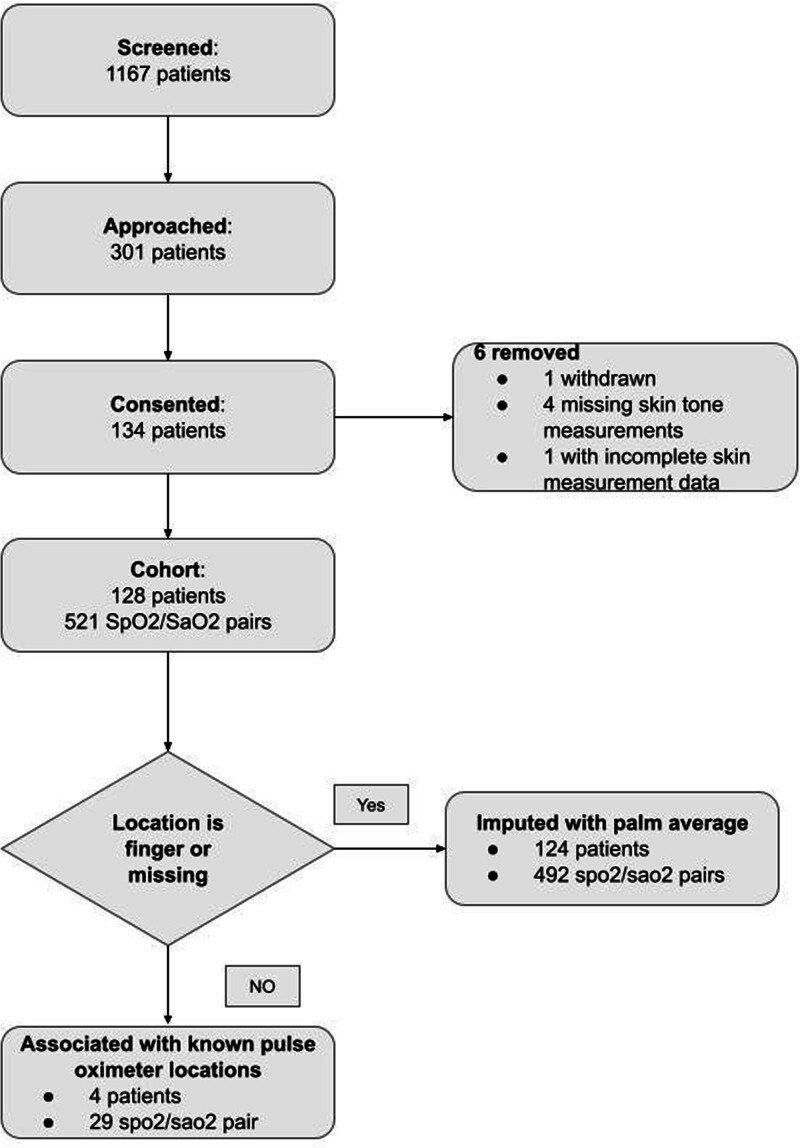
Measurements and main results: Sao2-Spo2 bias, variation of bias, and accuracy root mean square, comparing pulse oximetry, and ABG measurements. Linear mixed-effects models were fitted to estimate Sao2-Spo2 bias while accounting for clinical confounders.One hundred twenty-eight patients (57 Black, 56 White) with 521 ABG-pulse oximetry pairs were recruited. Skin tone data were prospectively collected using six measurement methods, generating eight measurements. The collected skin tone measurements were shown to yield differences among each other and overlap with self-reported racial groups, suggesting that skin tone could potentially provide information beyond self-reported race. Among the eight skin tone measurements in this study, and compared with self-reported race, the Monk Scale had the best relationship with differences in pulse oximetry bias (point estimate: -2.40%; 95% CI, -4.32% to -0.48%; p = 0.01) when comparing patients with lighter and dark skin tones.
Conclusions: We found clinical performance differences in pulse oximetry, especially in darker skin tones. Additional studies are needed to determine the relative contributions of skin tone measures and other potential factors on pulse oximetry discrepancies.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Wong holds equity and management roles in Ataia Medical. Dr. Wong is supported by the Duke CTSI by the National Center for Advancing Translational Sciences of the National Institutes of Health under UL1TR002553 and REACH Equity under the National Institute on Minority Health and Health Disparities of the National Institutes of Health under U54MD012530. Dr. Gichoya is a 2022 Robert Wood Johnson Foundation Harold Amos Medical Faculty Development Program and declares support from the RSNA Health Disparities grant (Number EIHD2204), Lacuna Fund (Number 67), Gordon and Betty Moore Foundation, and National Institutes of Health (National Institute of Biomedical Imaging and Bioengineering) Medical Imaging and Data Resource Center grant under contracts 75N92020C00008 and 75N92020C00021.
Figures
Update of
-
Utility of skin tone on pulse oximetry in critically ill patients: a prospective cohort study.medRxiv [Preprint]. 2024 Feb 27:2024.02.24.24303291. doi: 10.1101/2024.02.24.24303291. medRxiv. 2024. Update in: Crit Care Explor. 2024 Sep 11;6(9):e1133. doi: 10.1097/CCE.0000000000001133. PMID: 38464170 Free PMC article. Updated. Preprint.
References
-
- Charpignon M-L, Byers J, Cabral S, et al. : Critical bias in critical care devices. Crit Care Clin 2023; 39:795–813 - PubMed
-
- Jubran A, Tobin MJ: Reliability of pulse oximetry in titrating supplemental oxygen therapy in ventilator-dependent patients. Chest 1990; 97:1420–1425 - PubMed
-
- Nickerson BG, Sarkisian C, Tremper K: Bias and precision of pulse oximeters and arterial oximeters. Chest 1988; 93:515–517 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
