

NVL-655 Is a Selective and Brain-Penetrant Inhibitor of Diverse ALK-Mutant Oncoproteins, Including Lorlatinib-Resistant Compound Mutations
- PMID: 39269178
- PMCID: PMC11609626
- DOI: 10.1158/2159-8290.CD-24-0231
NVL-655 Is a Selective and Brain-Penetrant Inhibitor of Diverse ALK-Mutant Oncoproteins, Including Lorlatinib-Resistant Compound Mutations
Abstract
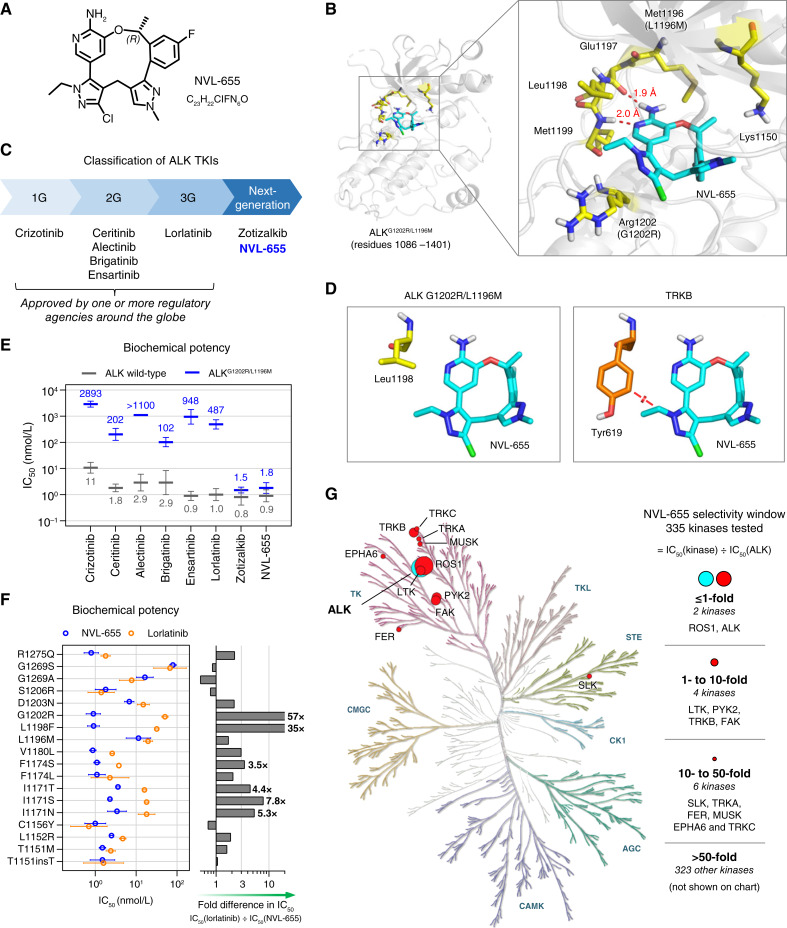
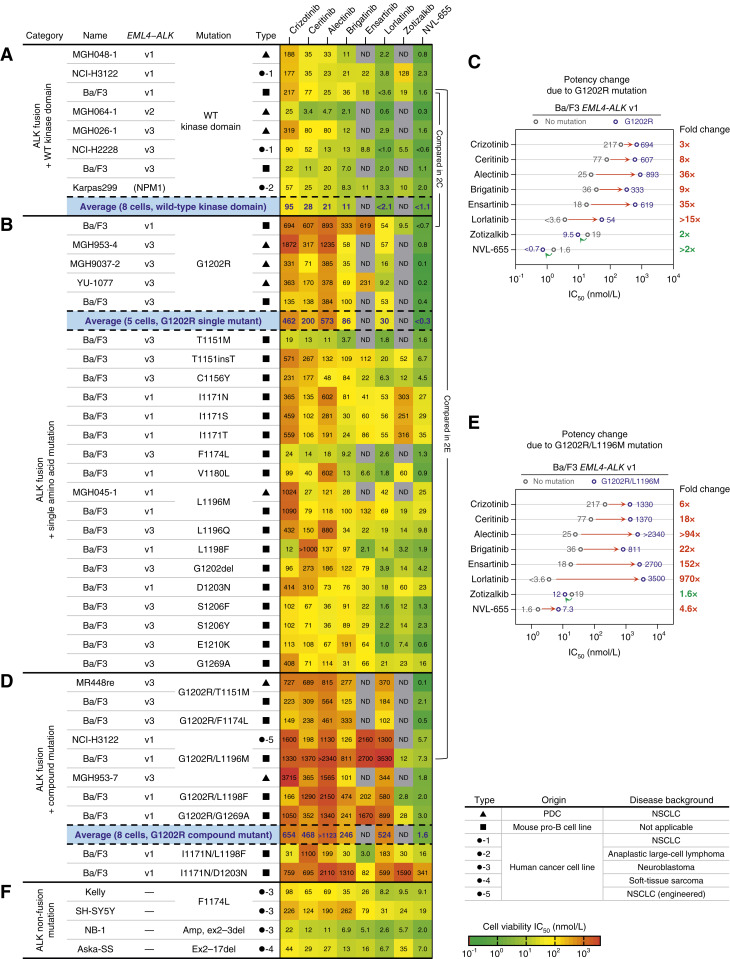
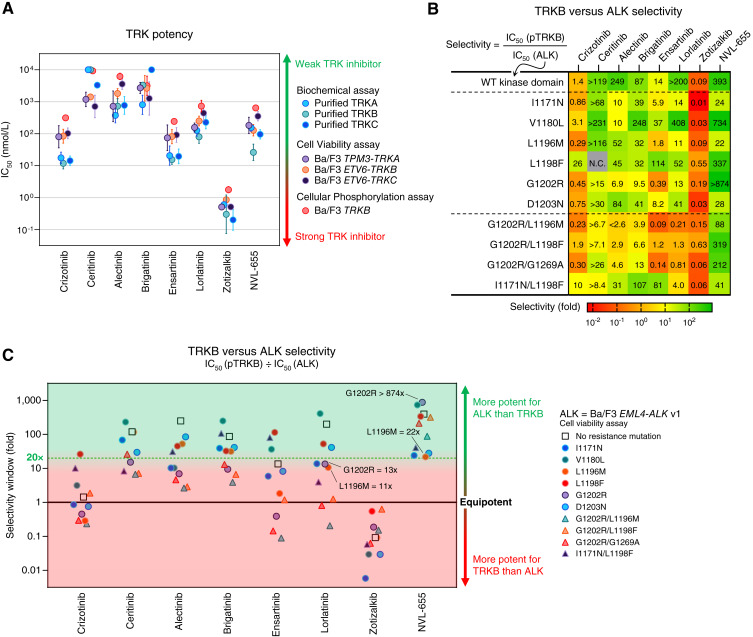
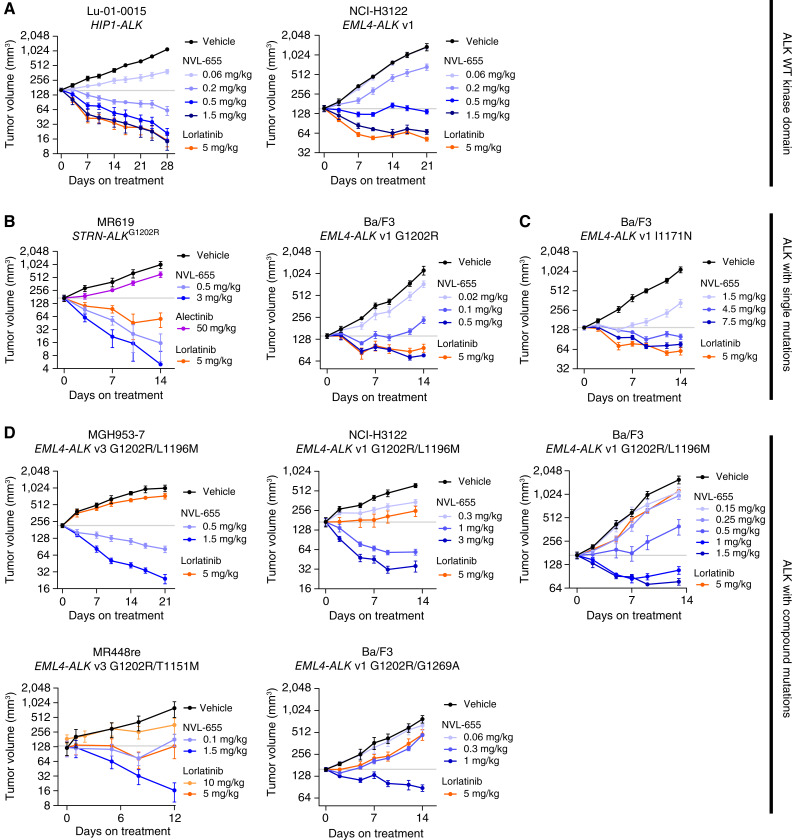
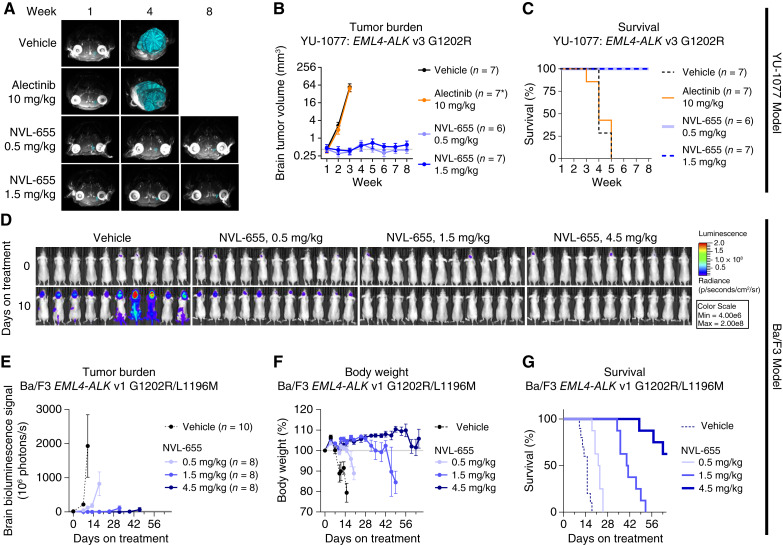
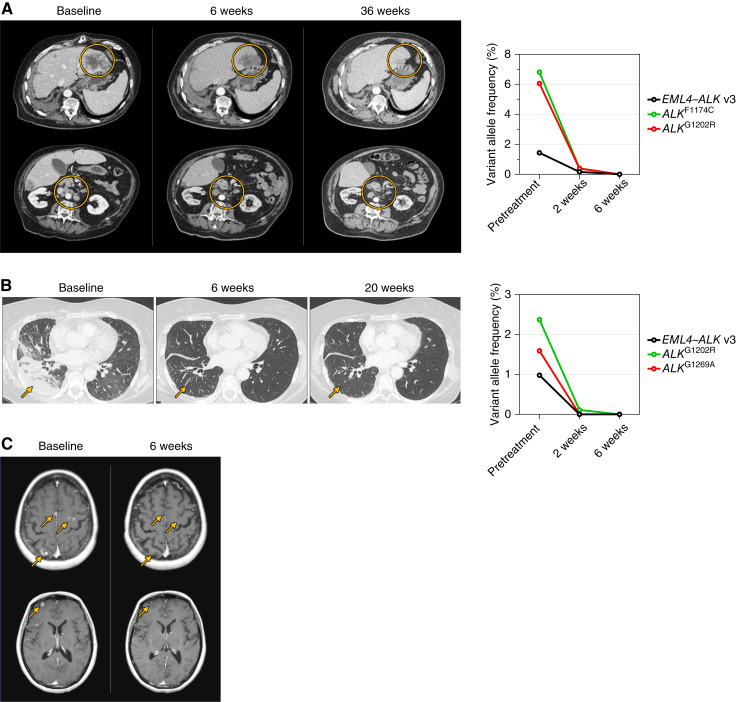
Three generations of tyrosine kinase inhibitors (TKI) have been approved for anaplastic lymphoma kinase (ALK) fusion-positive non-small cell lung cancer. However, none address the combined need for broad resistance coverage, brain activity, and avoidance of clinically dose-limiting TRK inhibition. NVL-655 is a rationally designed TKI with >50-fold selectivity for ALK over 96% of the kinome tested. In vitro, NVL-655 inhibits diverse ALK fusions, activating alterations, and resistance mutations, showing ≥100-fold improved potency against ALKG1202R single and compound mutations over approved ALK TKIs. In vivo, it induces regression across 12 tumor models, including intracranial and patient-derived xenografts. NVL-655 inhibits ALK over TRK with 22-fold to >874-fold selectivity. These preclinical findings are supported by three case studies from an ongoing first-in-human phase I/II trial of NVL-655 which demonstrate preliminary proof-of-concept clinical activity in heavily pretreated patients with ALK fusion-positive non-small cell lung cancer, including in patients with brain metastases and single or compound ALK resistance mutations. Significance: By combining broad activity against single and compound ALK resistance mutations, brain penetrance, and selectivity, NVL-655 addresses key limitations of currently approved ALK inhibitors and has the potential to represent a distinct advancement as a fourth-generation inhibitor for patients with ALK-driven cancers.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
J.J. Lin reports personal fees from C4 Therapeutics, Blueprint Medicines, Mirati Therapeutics, AnHeart Therapeutics, CLaiM Therapeutics, Regeneron, Yuhan, Ellipses Pharma, Daiichi Sankyo, AstraZeneca, and Hyku Biosciences, grants and personal fees from Genentech, Nuvalent, Bayer, Elevation Oncology, Novartis, Turning Point Therapeutics, and Bristol Myers Squibb, grants, personal fees, and other support from Pfizer, grants from Relay Therapeutics, Roche, and Linnaeus Therapeutics, and personal fees and other support from Merus outside the submitted work. J.C. Horan reports employment with and ownership interest in Nuvalent, Inc., and a patent for US11667649 granted, a patent for WO 2023/196900 pending, and a patent for WO 2024/086634 pending. A. Tangpeerachaikul reports employment with and ownership interest in Nuvalent, Inc., and a patent for US11667649 granted, a patent for WO 2023/196910 pending, and a patent for and a patent for WO 2024/086634 pending. M.L. Johnson reports grants from Nuvalent during the conduct of the study, as well as grants and other support from AbbVie, Amgen, Arcus Biosciences, ArriVent Biopharma, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly and Company, Fate Therapeutics, Genentech/Roche, Genmab, GlaxoSmithKline, Gritstone Oncology, Immunocore, Janssen, Merck, Mirati Therapeutics, Novartis, Pfizer, Revolution Medicines, Sanofi, and Takeda Pharmaceuticals, grants from Adaptimmune, Array BioPharma, Artios Pharma, Bayer, BeiGene, BerGenBio, BioAtla, Black Diamond, Calithera Biosciences, Carisma Therapeutics, City of Hope National Medical Center, Conjupro Biotherapeutics, Corvus Pharmaceuticals, Curis, CytomX, Dracen Pharmaceutical, Elicio Therapeutics, EMD Serono, EQRx, Erasca, Exelixis, Genocea Biosciences, Harpoon, Helsinn Healthcare, Hengrui Therapeutics, Hutchinson MediPharma, IDEAYA Biosciences, IGM Biosciences, Immuneering Corporation, Immunitas Therapeutics, IMPACT Therapeutics, Incyte, Kartos Therapeutics, LockBody Therapeutics, Loxo Oncology, Memorial Sloan Kettering, Merus, Mythic Therapeutics, NeoImmune Tech, Neovia Oncology, NextPoint Therapeutics, Numab Therapeutics, Nuvalent, OncoC4, Palleon Pharmaceuticals, PMV Pharmaceuticals, Rain Therapeutics, RasCal Therapeutics, Regeneron Pharmaceuticals, Relay Therapeutics, Ribon Therapeutics, Rubius Therapeutics, Seven and Eight Biopharmaceuticals, Shattuck Labs, Silicon Therapeutics, Summit Therapeutics, Syndax Pharmaceuticals, SystImmune, Taiho Oncology, TCR2 Therapeutics, Tempest Therapeutics, Theras, Tizona Therapeutics, Tmunity Therapeutics, Turning Point Therapeutics, Vividion, Vyriad, and Y-mAbs Therapeutics, and other support from Alentis Therapeutics, Biohaven Pharmaceuticals, D3 Bio Limited, Genmab, Gilead Sciences, Hookipa Biotech, Jazz Pharmaceuticals, ModeX Therapeutics, Molecular Axiom, Normunity, Novocure, Pyramid Biosciences, Seagen, Synthekine, Takeda Pharmaceuticals, and Zai Lab outside the submitted work. B. Besse reports other support from AbbVie, BioNTech SE, Bristol Myers Squibb, Chugai Pharmaceutical, CureVac AG, Daiichi Sankyo, F. Hoffmann-La Roche Ltd., PharmaMar, Regeneron, Sanofi Aventis, Turning Point Therapeutics, Eli Lilly and Company, Ellipses Pharma Ltd., Genmab, Immunocore, Janssen, MSD, Ose Immunotherapeutics, Owkin, Taiho oncology, BeiGene, Genmab A/S, GlaxoSmithKline, Janssen, Roche-Genentech, Sanofi, Takeda, Hedera Dx, and Springer Healthcare Ltd. during the conduct of the study. D.R. Camidge reports personal fees from Nuvalent, Pfizer, Takeda, and Roche during the conduct of the study. T. Fujino reports grants and personal fees from Nuvalent, Inc. during the conduct of the study; grants from Takeda Science Foundation, Eli Lilly Japan K.K., and Kinnate Biopharma Inc. outside the submitted work; and a patent for KU220115PCT pending. S. Yoda reports grants from Nuvalent, Inc. during the conduct of the study, as well as grants and personal fees from Nuvalent, Inc. and personal fees from Tango Therapeutics outside the submitted work. S. Mente reports employment with and ownership interest in Nuvalent, Inc., and a patent for US 11667649 granted. Y. Sun reports employment with and ownership interest in Nuvalent, Inc. N.E. Kohl reports personal fees from Nuvalent, Inc., during the conduct of the study; personal fees from M.D. Anderson Cancer Center, personal fees from ATPACAV LLC, outside the submitted work. J.R. Porter is a Board member and employee of and has ownership interest in Nuvalent, Inc., and a patent for WO 2023/196910 pending. M.D. Shair is a consultant/board member of and has ownership interest in Nuvalent, Inc. during the conduct of the study; has employment with Harvard University outside the submitted work; and reports a patent for US 11667649 granted. V.W. Zhu reports employment with and ownership interest in Nuvalent, Inc., and a patent for WO 2023/196910 pending. E. Felip reports other support from AbbVie, Amgen, AstraZeneca, Bayer, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly and Company, F. Hoffmann-La Roche, Genmab, Gilead, GSK, Janssen, Merck Serono, MSD, Novartis, Peptomyc, Pfizer, Regeneron, Sanofi, Takeda, Turning Point Therapeutics, Daiichi Sankyo, Genentech, Medical Trends, Medscape, PeerVoice, touchONCOLOGY, and Grifols outside the submitted work. B.C. Cho reports personal fees from Champions Oncology, Crown Bioscience, Imagen, PearlRiver Bio GmbH, Abion, BeiGene, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Bristol Myers Squibb, CJ Bioscience, CureLogen, Cyrus therapeutics, Ono Pharmaceutical, ONEGENE BIOTECHNOLOGY, Yuhan, Pfizer, Eli Lilly and Company, GI Cell, Guardant Health, HK inno.N, IMNEURUN Biosciences Inc., Janssen, Takeda, MSD, MedPacto, Blueprint Medicines, RandBio, Hanmi, Yonsei University Health System, Kanaph Therapeutic Inc., BridgeBio Therapeutics, Oscotec Inc., J INTS Bio, Therapex Co., Ltd., Gilead, Amgen, TheraCanVac Inc., Gencurix Inc., and Interpark Bio Convergence Corp., other support from DAAN Biotherapeutics, and grants from MOGAM Institute, LG Chem, Oscotec, Interpark Bio Convergence Corp., GI Innovation, GI Cell, Abion, AbbVie, AstraZeneca, Bayer, Blueprint Medicines, Boehringer Ingelheim, Champions Onocology, CJ Bioscience, CJ Blossom Park, Cyrus, Dizal Pharma, Genexine, Janssen, Eli Lilly and Company, MSD, Novartis, Nuvalent, Oncternal, Ono, Regeneron, Dong-A ST, BridgeBio Therapeutics, Yuhan, ImmuneOncia, Illumina, Kanaph Therapeutics, Therapex, J INTS BIO, Hanmi, CHA Bundang Medical Center, and Vertical Bio AG outside the submitted work. L. Friboulet reports grants from Nuvalent during the conduct of the study, as well as grants from Sanofi, Relay Therapeutics, and Amgen outside the submitted work. A.N. Hata reports grants and personal fees from Nuvalent during the conduct of the study, as well as grants and personal fees from Amgen and Pfizer, grants from BridgeBio, Bristol Myers Squibb, C4 Therapeutics, Eli Lilly and Company, Novartis, and Scorpion Therapeutics, and personal fees from Engine Biosciences, Oncovalent, TigaTx, and TOLREMO therapeutics outside the submitted work. H.E. Pelish reports employment with and ownership interest in Nuvalent, Inc., and a patent for US 11667649 granted, a patent for WO 2023/196910 pending, and a patent for WO 2024/086634 pending. A. Drilon reports personal fees from 14ner/Elevation Oncology, Amgen, AnHeart Therapeutics, AbbVie, ArcherDX, AstraZeneca, Bayer, BeiGene, BerGenBio, Blueprint Medicines, Boundless Bio, Bristol Myers Squibb, Chugai Pharmaceutical, EcoR1, EMD Serono, Entos, Exelixis, Helsinn, Hengrui Therapeutics, Ignyta/Genentech/Roche, InnoCare, Janssen, Loxo/Lilly, Merus, Monopteros, Monte Rosa, Novartis, Nuvalent, Pfizer, Prelude, Regeneron, Repare RX, Takeda/ARIAD/Millennium, Treeline Biosciences, TP Therapeutics, Tyra Biosciences, Verastem, Zymeworks, and MBrace and other support from Boehringer Ingelheim, Merck, and Puma during the conduct of the study; other support from Foundation Medicine, Teva, Taiho, GlaxoSmithKline, and PharmaMar and personal fees from Wolters Kluwer, and UpToDate Answers in CME, Applied Pharmaceutical Science, Inc., Axis, Clinical Care Options, Doc Congress, EPG Health, Harborside Nexus, i3 Health, IMEDEX, Liberum, Medendi, Medscape, Med Learning, Medtalks, MJH Life Sciences, MORE Health, Ology, OncLive, Paradigm, PeerView Institute, PeerVoice, Physicians’ Education Resources, Projects in Knowledge, Resources, Remedica Ltd., Research To Practice, RV More, Springer Healthcare, Targeted Oncology, Touch IME, and WebMD outside the submitted work; and a patent for selpercatinib osimertinib pending. No disclosures were reported by the other authors.
Figures
References
-
- Hallberg B, Palmer RH. The role of the ALK receptor in cancer biology. Ann Oncol 2016;27(Suppl 3):iii4–15. - PubMed
-
- Morris SW, Kirstein MN, Valentine MB, Dittmer KG, Shapiro DN, Saltman DL, et al. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science 1994;263:1281–4. - PubMed
-
- Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 2007;448:561–6. - PubMed
-
- Delsol G, Lamant L, Mariamé B, Pulford K, Dastugue N, Brousset P, et al. A new subtype of large B-cell lymphoma expressing the ALK kinase and lacking the 2; 5 translocation. Blood 1997;89:1483–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
