

Clinical multi-dimensional prognostic nomogram for predicting the efficacy of immunotherapy in NSCLC
- PMID: 39271765
- PMCID: PMC11399400
- DOI: 10.1038/s41598-024-72760-x
Clinical multi-dimensional prognostic nomogram for predicting the efficacy of immunotherapy in NSCLC
Abstract
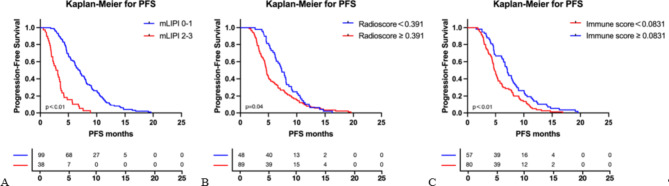
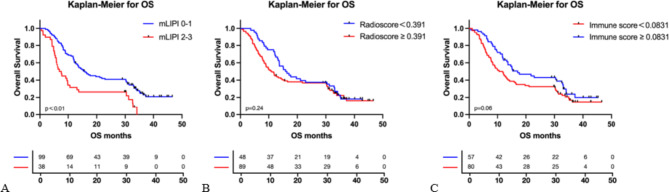
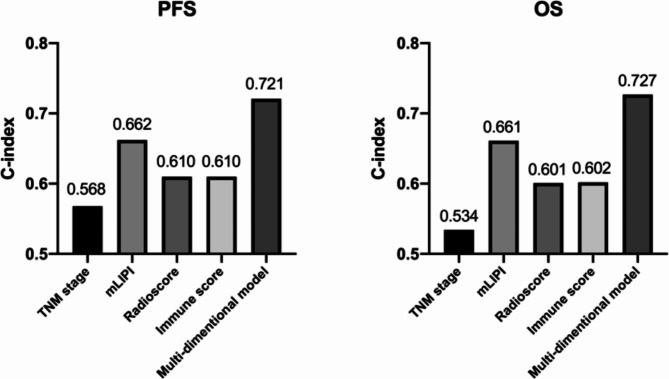
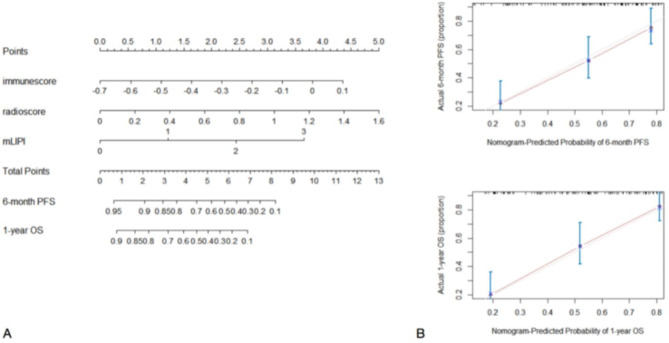
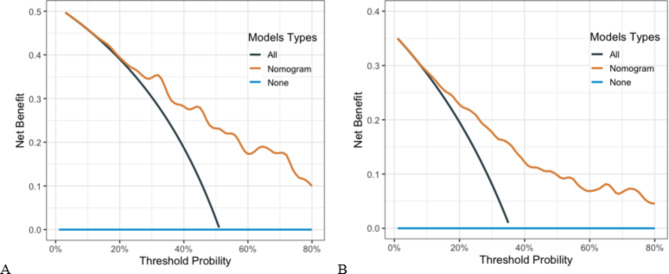
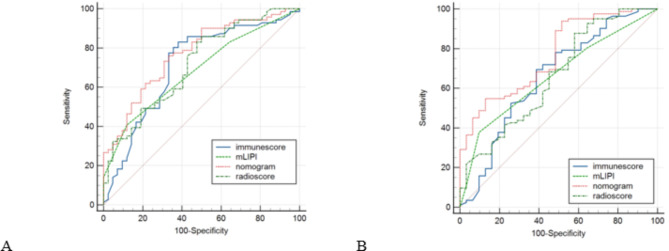
The advent of immunotherapy has greatly improved the prognosis of non-small cell lung (NSCLC) patients. However, given its low response rate and high cost of treatment, the search for valuable predictive markers of treatment efficacy is necessary. Considering the complexity and heterogeneity of the tumour and tumour microenvironment, the construction of a multi-dimensional prediction model is necessary. Therefore, we aimed to integrate clinical parameters, radiomic features, and immune signature data from NSCLC patients receiving immunotherapy to construct a multi-dimensional prediction model to better predict the efficacy of immunotherapy. The current study enrolled 137 NSCLC patients who received immunotherapy. We collected baseline clinical information, CT images, and tumour tissue specimens. Using 3D-Slicer software, radiomic features were extracted from patient CT images, and tumor tissue samples obtained before immunotherapy were subjected to immunohistochemical staining. Then, the least absolute shrinkage and selection operator (LASSO) Cox regression analysis was applied to downscale the data, and the radiomic features and immune signatures associated with the prognosis of immunotherapy patients were identified. The modified lung immune predictive index (mLIPI), radiomics score (Radioscore), immune score and multi-dimensional model nomogram were constructed. The C-index and area under the curve (AUC) were applied to evaluate the predictive efficacy of the models. Three radiomic features and three immune signatures that could predict the efficacy of immunotherapy were eventually screened. Multivariate analysis showed that the mLIPI, Radioscore, and immune score were independent predictive factors for PFS and OS (P < 0.05 for all models). The multi-dimensional model combining the three models showed better predictive efficacy than the mLIPI, Radioscore, and immune score (PFS: 0.721 vs. 0.662 vs. 0.610 vs. 0.610; OS: 0.727 vs. 0.661 vs. 0.601 vs. 0.602 respectively). The multi-dimensional model showed the best predictive efficacy, with C-index for PFS and OS higher than mLIPI, radioscore and immune score: 0.721 vs. 0.662 vs. 0.610 vs. 0.610 for PFS and 0.727 vs. 0.661 vs. 0.601 vs. 0.602 for OS, respectively. The AUC for the multi-dimensional model also performed better than those of the individual models: 0.771 vs. 0.684 vs. 0.715 vs. 0.711 for PFS and 0.768 vs. 0.662 vs. 0.661 vs. 0.658 for OS, respectively. The multi-dimensional model combining the three models had better predictive efficacy than any single model and was more likely to help provide patients personalized and precision medicine.
Keywords: Immunotherapy; Nomograms; Non-small cell lung cancer; Predictive; Radiomics.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
