

Trastuzumab deruxtecan in HER2-positive advanced breast cancer with or without brain metastases: a phase 3b/4 trial
- PMID: 39271844
- PMCID: PMC11645283
- DOI: 10.1038/s41591-024-03261-7
Trastuzumab deruxtecan in HER2-positive advanced breast cancer with or without brain metastases: a phase 3b/4 trial
Erratum in
-
Publisher Correction: Trastuzumab deruxtecan in HER2-positive advanced breast cancer with or without brain metastases: a phase 3b/4 trial.Nat Med. 2024 Dec;30(12):3780. doi: 10.1038/s41591-024-03349-0. Nat Med. 2024. PMID: 39653780 Free PMC article. No abstract available.
Abstract
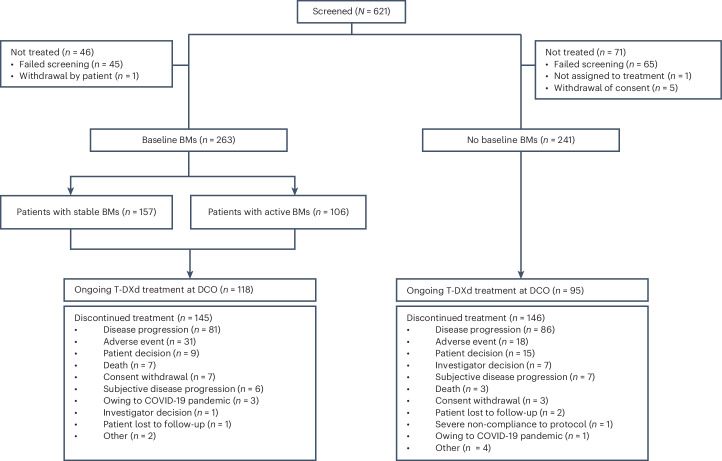
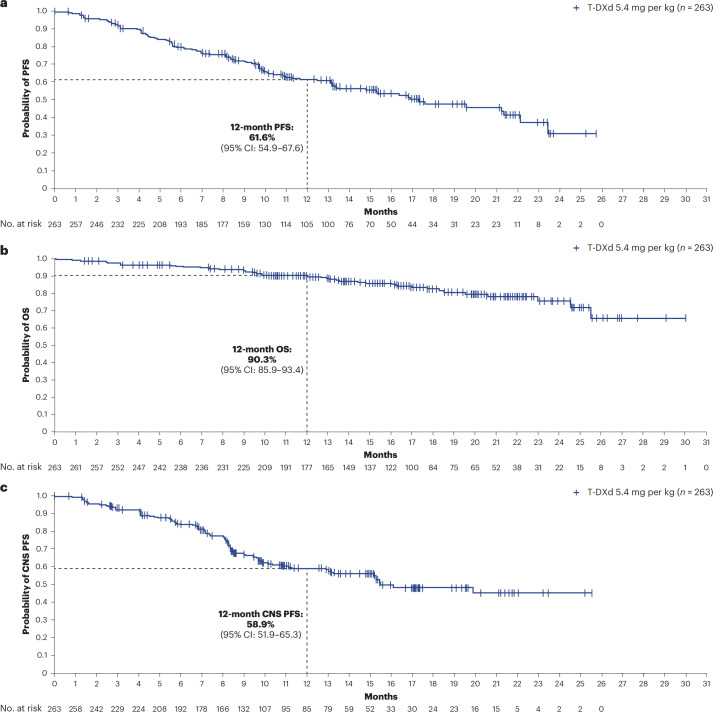
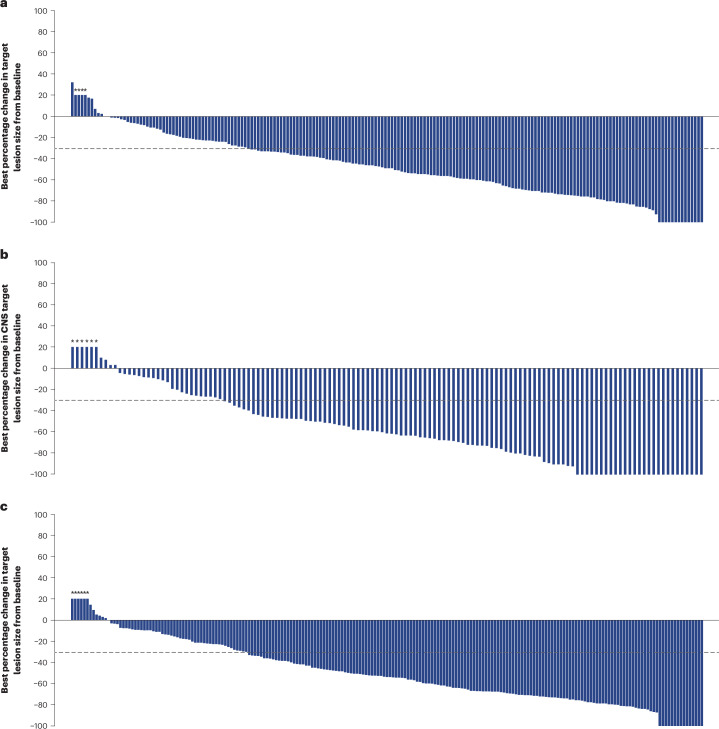
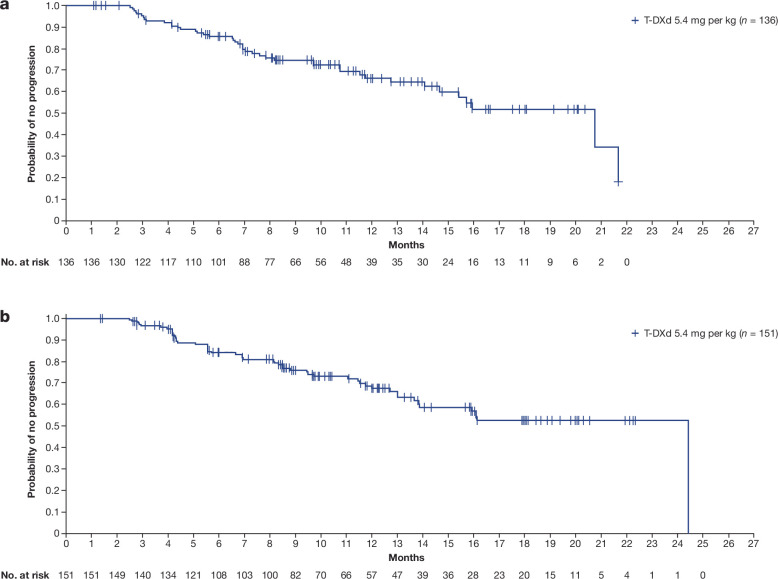
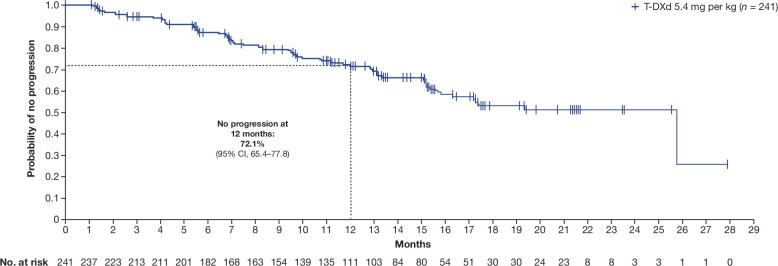
Trastuzumab deruxtecan (T-DXd) intracranial activity has been observed in small or retrospective patient cohorts with human epidermal growth factor receptor 2-positive (HER2+) advanced/metastatic breast cancer (mBC) and stable or active (untreated/previously treated and progressing) brain metastases (BMs). The phase 3b/4 DESTINY-Breast12 study investigated T-DXd in patients with HER2+ mBC and is, to our knowledge, the largest prospective study of T-DXd in patients with BMs in this setting. Patients (stable/active BMs (n = 263) and no BMs (n = 241)) treated with one or more prior anti-HER2-based regimens received T-DXd (5.4 mg per kg). Primary endpoints were progression-free survival (PFS; BMs cohort) and objective response rate (ORR) per Response Evaluation Criteria in Solid Tumors version 1.1 (non-BMs cohort). Additional endpoints included central nervous system (CNS) PFS, ORR, time to second progression, CNS ORR (BMs cohort), incidence of new symptomatic CNS metastases (non-BMs cohort), time to progression, duration of response, overall survival and safety (both cohorts). No formal hypothesis testing was conducted for this single-arm, open-label study. In the BMs cohort, 12-month PFS was 61.6% (95% confidence interval (CI): 54.9-67.6), and 12-month CNS PFS was 58.9% (95% CI: 51.9-65.3). In the non-BMs cohort, ORR was 62.7% (95% CI: 56.5-68.8). Grade 3 or higher adverse events occurred in 51% (BMs cohort) and 49% (non-BMs cohort) of patients. Investigator-reported interstitial lung disease/pneumonitis occurred in 16% (grade ≥3: 3%) of patients with BMs and 13% (grade ≥3: 1%) of patients without BMs. These data show substantial and durable overall and intracranial activity for T-DXd, supporting its use in previously treated patients with HER2+ mBC irrespective of stable/active baseline BMs. ClinicalTrials.gov identifier: NCT04739761 .
© 2024. The Author(s).
Conflict of interest statement
Competing interests: N.H. has received lecture honoraria from Art Tempi, AstraZeneca, Daiichi Sankyo, Eli Lilly, Gilead Sciences, Medscape, Merck Sharp & Dohme, Novartis, Onkowissen, Pierre Fabre, Roche, Sanofi, Seagen, Viatris and Zuellig Pharma; has received consulting or advisory honoraria from Aptitude Health, Gileadn Sciences, Pfizer, Sandox-Hexal, Sanofi and Seagen; has received research funding from AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Gilead Sciences, Merck Sharp & Dohme, Roche, Seagen, TRIO and WSG; has participated on independent data monitoring committees/steering committees for Eli Lilly, Pierre Fabre and Roche; and has ownership interest in the West German Study Group. E.C. has received lecture, consulting or advisory honoraria from AstraZeneca, Daiichi Sankyo, Eli lilly, Gilead Sciences, Menarini, Merck Sharp & Dohme, Novartis, Pfizer, Reveal Genomics and Roche; has received support for attending meetings and/or travel from AstraZeneca, Pfizer and Roche; has received research funding from Daiichi Sankyo, Pfizer and Roche; and has participated on steering committees for AstraZeneca, Daiichi Sankyo, Gilead Sciences, Novartis, Reveal Genomics and Roche. G.J. has received consulting honoraria from AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Diaccurate/Evexta Bio, Eli Lilly, Novartis, Pfizer, Roche and Seagen; has received honoraria from AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Novartis, Pfizer, Roche and Seagen; has received support for attending meetings and/or travel from Amgen, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Gilead Sciences, Novartis, Pfizer and Roche; and has received medical writing support from Amgen, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Novartis and Roche. V.M. has received lecture honoraria from AstraZeneca, Daiichi Sankyo, Eisai, Gilead Sciences, high5 Oncology, iMED Institut, Eli Lilly, Medac, Medscape, Merck Sharp & Dohme, Novartis, Onkowissen, Pfizer, Pierre Fabre, Roche and Seagen; has received consulting or advisory honoraria from ClinSol, Daiichi Sankyo, Eisai, Eli Lilly, Gilead Sciences, Menarini Stemline, Merck Sharp & Dohme, Novartis, Pierre Fabre, PINK, Roche and Menarini Stemline; and has received research funding from AstraZeneca, Genentech, Novartis, Roche and Seagen. N.N. has received consulting or advisory honoraria from AstraZeneca, Chugai Pharmaceutical and Daiichi Sankyo; has received lecture honoraria from AstraZeneca, Chugai Pharmaceutical, Eisai, Daiichi Sankyo, Eli Lilly Japan, Nippon Kayaku and Pfizer Japan; and has received research funding from Chugai Pharmaceutical, Daiichi Sankyo, Eli Lilly Japan, Nippon Kayaku and Pfizer Japan. G.V. has received research grants from Dako/Agilent Technologies, Roche/Genentech and Ventana Medical Systems and has received honoraria from AstraZeneca, Daiichi Sankyo, Dako/Agilent Technologies, Gilead Sciences, Merck Sharp & Dohme Oncology, Pfizer, Roche and Ventana Medical Systems. R.B. has held advisory roles at AstraZeneca, Daiichi Sankyo, Eisai, Eli Lilly, Gilead Sciences, Grünenthal, Merck Sharp & Dohme, Novartis, Pfizer, Pierre Fabre, Roche, Seagen and Menarini Stemline; has received lecture honoraria from AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Eisai, Eli Lilly, Gilead Sciences, Grünenthal, Menarini Stemline, Merck Sharp & Dohme, Novartis, Pfizer, Pierre Fabre, Roche and Seagen; and has received research support from Daiichi Sankyo, Merck Sharp & Dohme, Novartis and Roche. C.K. has received lecture honoraria from AstraZeneca, Eli Lilly, Genomic Health/Exact Sciences, Gilead Sciences, GlaxoSmithKline, Novartis, PharmaMar, Pfizer and Roche; has received consulting or advisory honoraria from AstraZeneca, Eli Lilly, Genomic Health/Exact Sciences, Gilead Sciences, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, PharmaMar and Roche; and has participated on steering committees for AstraZeneca. M.J.H. has received lecture honoraria from AstraZeneca. R.M.C. received an unrestricted educational grant from Pfizer; has received research support from AstraZeneca, Daiichi Sankyo, MSD Ireland and Pfizer; has received honoraria from AstraZeneca, Daiichi Sankyo, Eli Lilly, Gilead Sciences and Seagen; and has received support for attending meetings and/or travel from Gilead Sciences, Novartis and Roche. M.G. has received support for attending meetings and/or travel from AstraZeneca, Gilead Sciences, Roche and Pfizer and has received honoraria from AstraZeneca, Gilead Sciences and Pfizer. V.G. has received honoraria from AstraZeneca, Daiichi Sankyo, Eli Lilly, Exact Sciences, Gilead Sciences, Menarini Stemline, Merck Sharp & Dohme, Novartis, Pfizer, Olema Oncology, Pierre Fabre and Roche; has received lecture honoraria from AstraZeneca, Daiichi Sankyo, Eli Lilly, Exact Sciences, Gilead Sciences, GlaxoSmithKline, Menarini Stemline, Novartis, Roche and Zentiva; and has received expert testimony honoraria from Eli Lilly. G.B. has received honoraria from Agendia, Amgen, AstraZeneca, Chugai Pharmaceutical/Roche, Daiichi Sankyo, Eisai, Exact Sciences, Gilead Sciences, Helsinn Lilly, Menarini Stemline, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Sanofi and Seagen and received a research grant from Gilead Sciences. H.W. has received lecture honoraria from Seagen; has received consulting or advisory honoraria from AstraZeneca, Augustine Therapeutics, Daiichi Sankyo, E Squared Communications, Eli Lilly, Gilead Sciences, Immutep, MediMix, Menarini Stemline, Novartis, NV Hict, Pfizer, PSI CRO and Roche; has received support for attending meetings and/or travel from Daiichi Sankyo and Pfizer; has received research funding from Novartis, Roche and Syneos Health; and has received subscription fees from Gilead Sciences. S.E.-d.-R. has received honoraria from AstraZeneca, COR2ED, Daiichi Sankyo, Jazz Pharmaceuticals, Medistream, Pierre Fabre, Roche and Seagen; has received research funding from AstraZeneca, Byondis, Daiichi Sankyo, Jazz Pharmaceuticals, MEDSIR, Roche, SOLTI and Zymeworks; and has received support for attending meetings and/or travel from AstraZeneca, Daiichi Sankyo, Kern Pharma, Pfizer, Seagen and SOLTI. M.P., H.B., N.K.-C., N.S. and S.V. are employees of AstraZeneca. N.K.-C. holds stocks in AstraZeneca and AbbVie. N.U.L. has received honoraria from AstraZeneca and has received research funding from AstraZeneca. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
