

Prevalence of cardiovascular events in a population-based registry of patients with systemic lupus erythematosus
- PMID: 39272198
- PMCID: PMC11401284
- DOI: 10.1186/s13075-024-03395-6
Prevalence of cardiovascular events in a population-based registry of patients with systemic lupus erythematosus
Abstract
Background: The Manhattan Lupus Surveillance Program (MLSP), a population-based retrospective registry of patients with systemic lupus erythematosus (SLE), was used to investigate the prevalence of cardiovascular disease events (CVE) and compare rates among sex, age and race/ethnicity to population-based controls.
Methods: Patients with prevalent SLE in 2007 aged ≥ 20 years in the MLSP were included. CVE required documentation of a myocardial infarction or cerebrovascular accident. We calculated crude risk ratios and adjusted risk ratios (ARR) controlling for sex, age group, race and ethnicity, and years since diagnosis. Data from the 2009-2010 National Health and Nutrition Examination Survey (NHANES) and the 2013-2014 NYC Health and Nutrition Examination Survey (NYC HANES) were used to calculate expected CVE prevalence by multiplying NHANES and NYC HANES estimates by strata-specific counts of patients with SLE. Crude prevalence ratios (PRs) using national and NYC estimates and age standardized prevalence ratios (ASPRs) using national estimates were calculated.
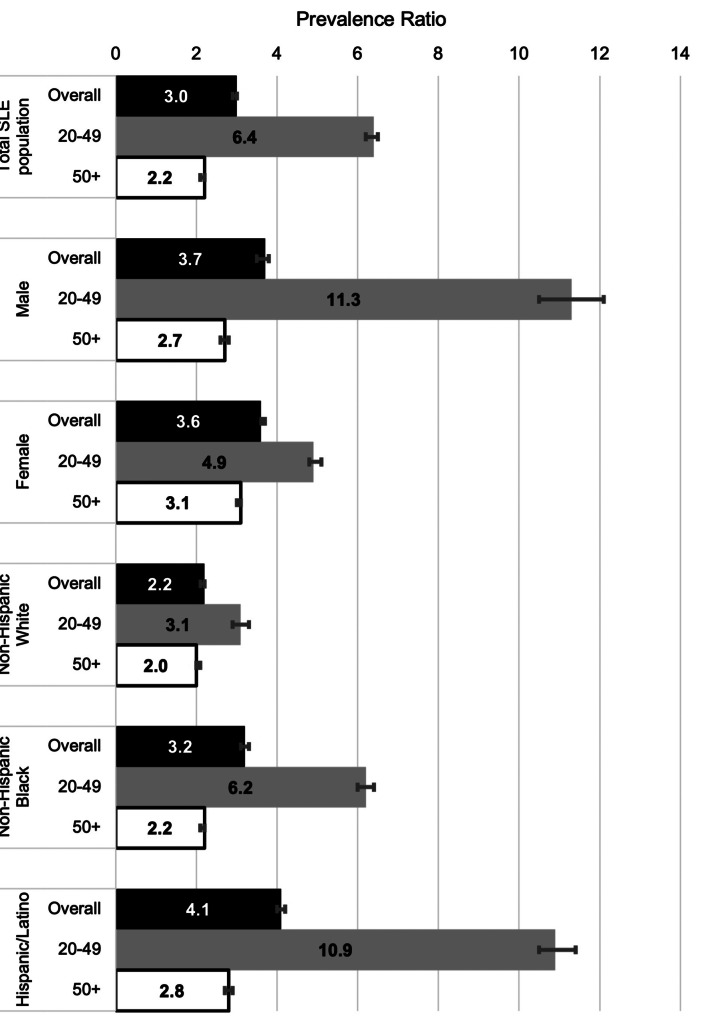
Results: CVE occurred in 13.9% of 1,285 MLSP patients with SLE, and risk was increased among men (ARR:1.7, 95%CI:1.2-2.5) and older adults (age > 60 ARR:2.5, 95%CI:1.7-3.8). Compared with non-Hispanic Asian patients, CVE risk was elevated among Hispanic/Latino (ARR:3.1, 95%CI:1.4-7.0) and non-Hispanic Black (ARR:3.5, 95%CI1.6-7.9) patients as well as those identified as non-Hispanic and in another or multiple racial groups (ARR:4.2, 95%CI:1.1-15.8). Overall, CVE prevalence was higher among patients with SLE than nationally (ASPR:3.1, 95%CI:3.0-3.1) but did not differ by sex. Compared with national race and ethnicity-stratified estimates, CVE among patients with SLE was highest among Hispanics/Latinos (ASPR:4.3, 95%CI:4.2-4.4). CVE was also elevated among SLE registry patients compared with all NYC residents. Comparisons with age-stratified national estimates revealed PRs of 6.4 (95%CI:6.2-6.5) among patients aged 20-49 years and 2.2 (95%CI:2.1-2.2) among those ≥ 50 years. Male (11.3, 95%CI:10.5-12.1), Hispanic/Latino (10.9, 95%CI:10.5-11.4) and non-Hispanic Black (6.2, 95%CI:6.0-6.4) SLE patients aged 20-49 had the highest CVE prevalence ratios.
Conclusions: These population-based estimates of CVE in a diverse registry of patients with SLE revealed increased rates among younger male, Hispanic/Latino and non-Hispanic Black patients. These findings reinforce the need to appropriately screen for CVD among all SLE patients but particularly among these high-risk patients.
Keywords: Cardiovascular disease; Cerebrovascular accident; Epidemiology; Myocardial infarction; Systemic lupus erythematosus.
© 2024. The Author(s).
Conflict of interest statement
PMI - consulting fees from GSK, Momenta/Janssen, Hansoh Bio; JPB - consulting fees from Bristol-Myers Squibb, GlaxoSmithKline, Related Sciences LLC, Ventus Therapeutics, Artiva; and CG - consulting fees from Alumis, Amgen, Astra-Zeneca, Sanofi, and UCB.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
