

Neuroimaging in Nonsyndromic Craniosynostosis: Key Concepts to Unlock Innovation
- PMID: 39272627
- PMCID: PMC11394062
- DOI: 10.3390/diagnostics14171842
Neuroimaging in Nonsyndromic Craniosynostosis: Key Concepts to Unlock Innovation
Abstract
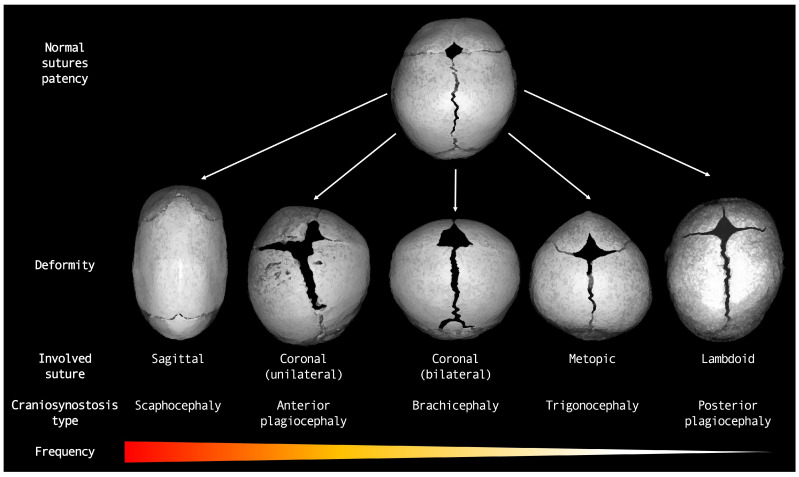
Craniosynostoses (CRS) are caused by the premature fusion of one or more cranial sutures, with isolated nonsyndromic CRS accounting for most of the clinical manifestations. Such premature suture fusion impacts both skull and brain morphology and involves regions far beyond the immediate area of fusion. The combined use of different neuroimaging tools allows for an accurate depiction of the most prominent clinical-radiological features in nonsyndromic CRS but can also contribute to a deeper investigation of more subtle alterations in the underlying nervous tissue organization that may impact normal brain development. This review paper aims to provide a comprehensive framework for a better understanding of the present and future potential applications of neuroimaging techniques for evaluating nonsyndromic CRS, highlighting strategies for optimizing their use in clinical practice and offering an overview of the most relevant technological advancements in terms of diagnostic performance, radiation exposure, and cost-effectiveness.
Keywords: arterial spin labeling; blackbone MRI; computed tomography; craniofacial surgery; craniosynostosis; magnetic resonance angiography; magnetic resonance imaging; neuroradiology; perfusion MRI.
Conflict of interest statement
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
