

Post-Thrombectomy Subarachnoid Hemorrhage: Incidence, Predictors, Clinical Relevance, and Effect Modulators
- PMID: 39272641
- PMCID: PMC11394096
- DOI: 10.3390/diagnostics14171856
Post-Thrombectomy Subarachnoid Hemorrhage: Incidence, Predictors, Clinical Relevance, and Effect Modulators
Abstract
Background: Subarachnoid hemorrhage (SAH) following endovascular thrombectomy (EVT) is a poorly understood phenomenon, and whether it is associated with clinical detriment is unclear.
Methods: This was an explorative analysis of a national database of real-world hospitalizations in the United States. Patients who underwent EVT were included. Patients were divided into SAH and non-SAH groups, and hospitalization outcomes were compared using multivariable logistic regression models. Regression models were also used to identify significant predictors for post-EVT SAH, and significant modulators of SAH's association with hospitalization outcomes were also assessed.
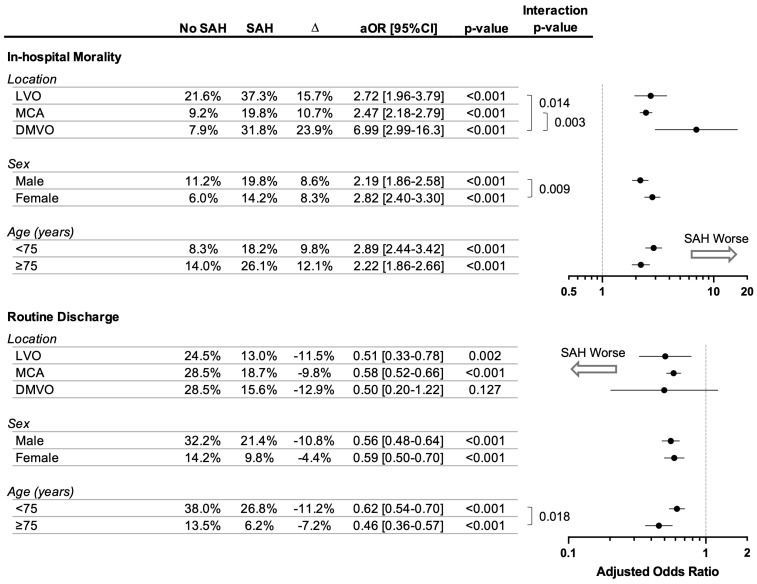
Results: A total of 99,219 EVT patients were identified; 6174 (6.2%) had SAH. Overall, SAH was independently associated with increased odds of in-hospital mortality (21.5% vs. 10.6%, adjusted OR 2.53 [95%CI 2.23-2.87], p < 0.001) and lower odds of routine discharge to home with self-care (18.2% vs. 28.0%, aOR 0.58 [95%CI 0.52-0.65], p < 0.001). Distal/medium vessel occlusion (DMVO), coagulopathy, angioplasty or stenting, concurrent intraparenchymal hemorrhage (IPH), and female sex were associated with higher odds of SAH. DMVO was associated with particularly heightened risk of death (31.8% vs. 7.9%, aOR 6.99 [95%CI 2.99 to 16.3], p < 0.001), which was an effect size significantly larger than other sites of vascular occlusion (interaction p > 0.05).
Conclusion: SAH is an uncommon but likely clinically detrimental post-EVT complication. DMVO, coagulopathy, angioplasty or stenting, concurrent IPH, and female sex were independently associated with higher odds of post-EVT SAH. SAH associated with DMVO-EVT may be particularly harmful.
Keywords: distal; endovascular; intracranial hemorrhage; medium; stroke; subarachnoid hemorrhage; thrombectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Powers W.J., Rabinstein A.A., Ackerson T., Adeoye O.M., Bambakidis N.C., Becker K., Biller J., Brown M., Demaerschalk B.M., Hoh B., et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. - PubMed
-
- Turc G., Bhogal P., Fischer U., Khatri P., Lobotesis K., Mazighi M., Schellinger P.D., Toni D., de Vries J., White P., et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischemic Stroke. J. Neurointerv. Surg. 2023;15:e8. doi: 10.1136/neurintsurg-2018-014569. - DOI - PubMed
LinkOut - more resources
Full Text Sources
