

Escalation and De-Escalation of Adjuvant Radiotherapy in Early Breast Cancer: Strategies for Risk-Adapted Optimization
- PMID: 39272804
- PMCID: PMC11394564
- DOI: 10.3390/cancers16172946
Escalation and De-Escalation of Adjuvant Radiotherapy in Early Breast Cancer: Strategies for Risk-Adapted Optimization
Abstract
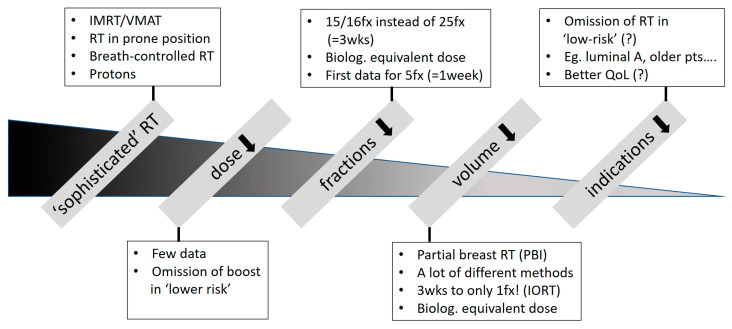
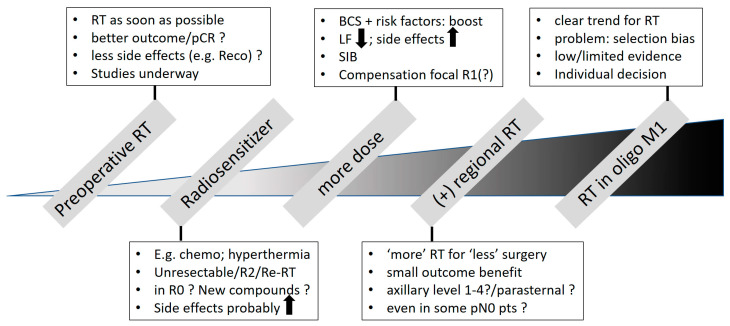
Postoperative radiotherapy (RT) is recommended after breast-conserving surgery and mastectomy (with risk factors). Consideration of pros and cons, including potential side effects, demands the optimization of adjuvant RT and a risk-adapted approach. There is clear de-escalation in fractionation-hypofractionation should be considered standard. For selected low-risk situations, PBI only or even the omission of RT might be appropriate. In contrast, tendencies toward escalating RT are obvious. Preoperative RT seems attractive for patients in whom breast reconstruction is planned or for defining the tumor location more precisely with the potential of giving ablative doses. Dose escalation by a (simultaneous integrated) boost or the combination with new compounds/systemic treatments may increase antitumor efficacy but also toxicity. Despite low evidence, RT for oligometastatic disease is becoming increasingly popular. The omission of axillary dissection in node-positive disease led to an escalation of regional RT. Studies are ongoing to test if any axillary treatment can be omitted and which oligometastatic patients do really benefit from RT. Besides technical improvements, the incorporation of molecular risk profiles and also the response to neoadjuvant systemic therapy have the potential to optimize the decision-making concerning if and how local and/or regional RT should be administered.
Keywords: adjuvant radiotherapy; de-escalation; escalation; loco-regional irradiation; omission of radiotherapy; optimization; partial breast irradiation.
Conflict of interest statement
Guenther Gruber has no conflicts of interest to declare.
Figures
References
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Darby S., McGale P., Correa C., Taylor C., Arriagada R., Clarke M., Cutter D., Davies C., Ewertz M., et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707–1716. - PMC - PubMed
-
- Shariati S., Behroozian T., Kennedy S., Caini S., Herst P.M., Zhang L., Ding K., Karam I., van den Hurk C., Wolf J.R., et al. Mepithel film for the prevention and treatment of acute radiation dermatitis in breast cancer: A systematic review and meta-analysis of randomized controlled trials. Support Care Cancer. 2023;31:524. doi: 10.1007/s00520-023-07982-2. - DOI - PubMed
-
- Prescott R.J., Kunkler I.H., Williams L.J., King C.C., Jack W., van der Pol M., Goh T.T., Lindley R., Cairns J. A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial. Health Technol. Assess. 2007;11:1–149. doi: 10.3310/hta11310. - DOI - PubMed
-
- Velikova G., Williams L.J., Willis S., Dixon J.M., Loncaster J., Hatton M., Clarke J., Kunkler I.H., Russell N.S., MRC SUPREMO Trial UK Investigators Quality of life after postmastectomy radiotherapy in patients with intermediate-risk breast cancer (SUPREMO): 2-year follow-up results of a randomised controlled trial. Lancet Oncol. 2018;19:1516–1529. doi: 10.1016/S1470-2045(18)30515-1. - DOI - PubMed
-
- Joseph K., Vos L.J., Gabos Z., Pervez N., Chafe S., Tankel K., Warkentin H., Ghosh S., Amanie J., Powell K., et al. Skin Toxicity in Early Breast Cancer Patients Treated with Field-In-Field Breast Intensity-Modulated Radiotherapy versus Helical Inverse Breast Intensity-Modulated Radiotherapy: Results of a Phase III Randomised Controlled Trial. Clin. Oncol. (R. Coll. Radiol.) 2021;33:30–39. doi: 10.1016/j.clon.2020.07.005. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
