

Establishing Treatment Effectiveness in Fabry Disease: Observation-Based Recommendations for Improvement
- PMID: 39273698
- PMCID: PMC11396259
- DOI: 10.3390/ijms25179752
Establishing Treatment Effectiveness in Fabry Disease: Observation-Based Recommendations for Improvement
Abstract
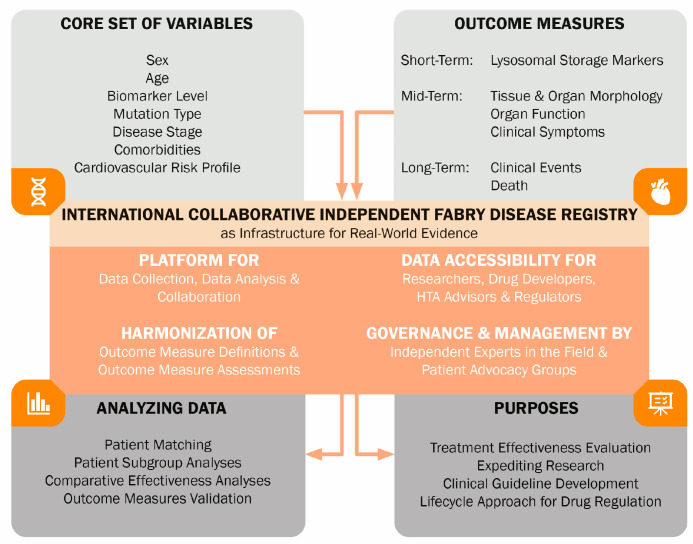
Fabry disease (FD, OMIM #301500) is caused by pathogenic GLA gene (OMIM #300644) variants, resulting in a deficiency of the α-galactosidase A enzyme with accumulation of its substrate globotriaosylceramide and its derivatives. The phenotype of FD is highly variable, with distinctive disease features and course in classical male patients but more diverse and often nonspecific features in non-classical and female patients. FD-specific therapies have been available for approximately two decades, yet establishing robust evidence for long-term effectiveness remains challenging. This review aims to identify the factors contributing to this lack of robust evidence for the treatment of FD with enzyme replacement therapy (ERT) (agalsidase-alfa and -beta and pegunigalsidase alfa) and chaperone therapy (migalastat). Major factors that have been identified are study population heterogeneity (concerning sex, age, phenotype, disease stage) and differences in study design (control groups, outcomes assessed), as well as the short duration of studies. To address these challenges, we advocate for patient matching to improve control group compatibility in future FD therapy studies. We recommend international collaboration and harmonization, facilitated by an independent FD registry. We propose a stepwise approach for evaluating the effectiveness of novel treatments, including recommendations for surrogate outcomes and required study duration.
Keywords: Fabry disease; chaperone therapy; clinical outcomes; enzyme replacement therapy (ERT); treatment effectiveness.
Conflict of interest statement
B.C.F.V. is involved in a premarketing study with Sanofi-Genzyme. Financial arrangements were made through AMC Research BV. No fees, travel support, or grants were obtained from the Pharmaceutical Industry. M. Langeveld is involved in premarketing studies with Sanofi-Genzyme and Protalix/Chiesi. Financial arrangements were made through AMC Research BV. No fees, travel support, or grants were obtained from the Pharmaceutical Industry. D.H.S., L.v.D., and M.R.D. declare that they have no conflicts of interest.
Figures

References
-
- Metha A., Hughes D.A. Fabry Disease. [(accessed on 1 June 2024)]; Available online: https://www.ncbi.nlm.nih.gov/books/NBK1292/
-
- van der Veen S.J., Sayed M.E., Hollak C.E.M., Brands M.M., Snelder C.K.S., Boekholdt S.M., Vogt L., Goorden S.M.I., van Kuilenburg A.B.P., Langeveld M. Early Risk Stratification for Natural Disease Course in Fabry Patients Using Plasma Globotriaosylsphingosine Levels. Clin. J. Am. Soc. Nephrol. 2023;18:1272–1282. doi: 10.2215/CJN.0000000000000239. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
