

Perfecting the pour: A novel co-axial technique with sequential injections for optimising cement delivery during sacroplasty
- PMID: 39275844
- PMCID: PMC11559721
- DOI: 10.1177/15910199241282709
Perfecting the pour: A novel co-axial technique with sequential injections for optimising cement delivery during sacroplasty
Abstract
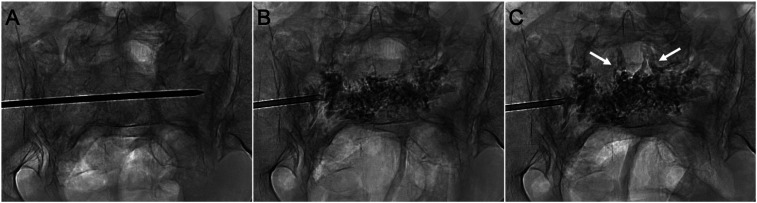
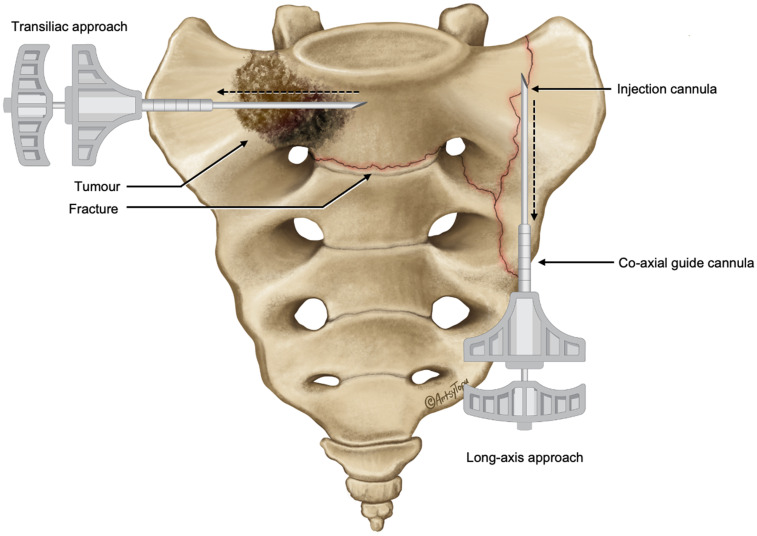
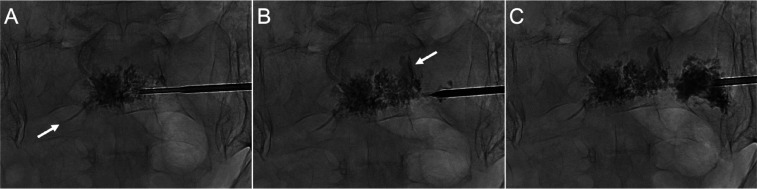
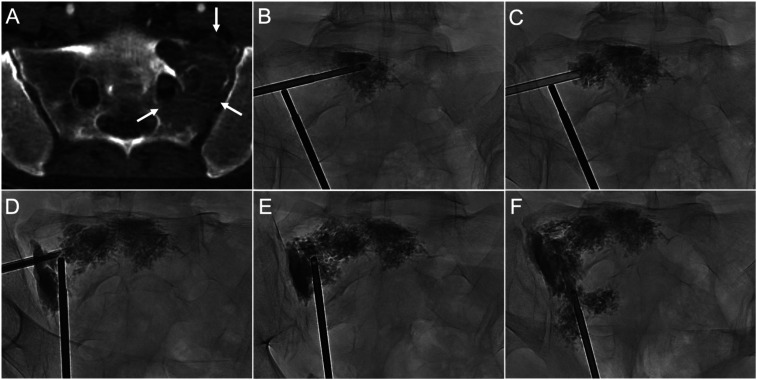
Background: Percutaneous sacroplasty is an effective treatment for painful sacral fractures and tumours, however there is no accepted optimal technique for performing this procedure. This study investigated a novel approach to sacroplasty combining co-axial sacral access, sequential cement injections and hypothermic cement manipulation to improve cement delivery.
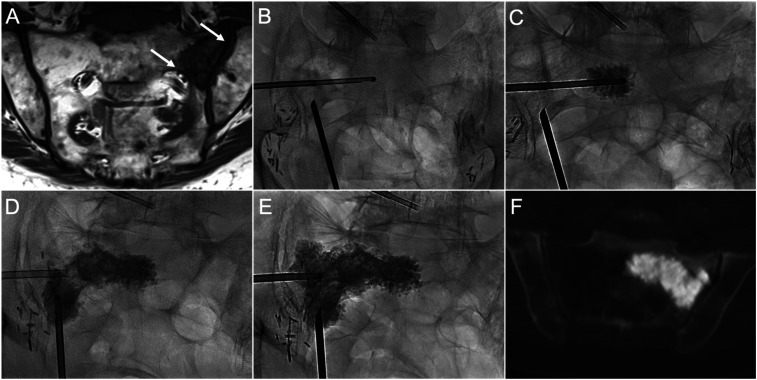
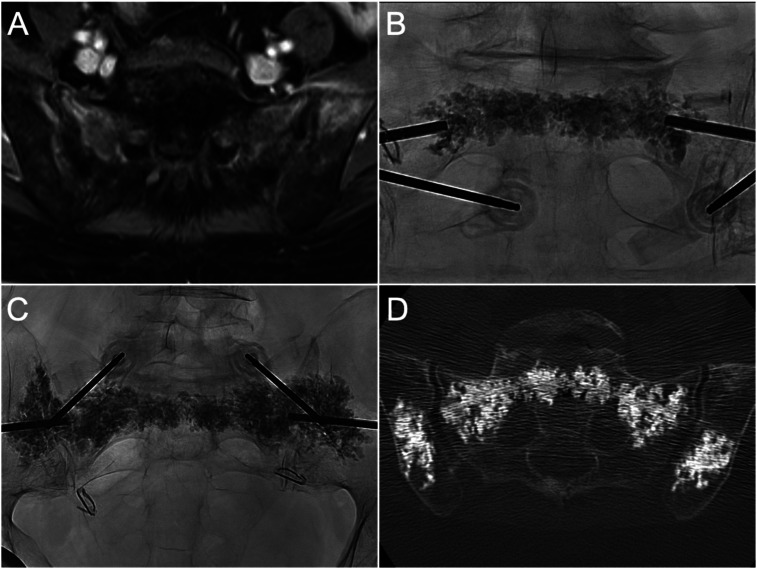
Methods: This retrospective study analysed 11 patients who underwent co-axial sacroplasty between April 2023 and March 2024 for treatment of painful insufficiency fractures (n = 5) or malignant sacral tumours (n = 6). All cases were performed using biplane fluoroscopy with conebeam CT navigation for planning and monitoring percutaneous access. Procedural details, technical outcomes, and clinical outcomes including Numerical Rating Scale (NRS) pain and analgesic utilisation on a six-point scale were analysed pre-procedure and at follow-up.
Results: Technical success of was achieved in all cases using this technique. The mean injected cement volume was 20.5 ± 6.4 ml. Median pre-procedural NRS pain scores of 8 (IQR 7.25-8) significantly decreased to 0 (IQR, 0-0.25) at follow-up (p <.01). The median preprocedural analgesic utilisation score reduced from 3 (IQR, 2-3) to 0 (IQR, 0-2.5) at follow-up (p <.01). Cement leakage occurred during two cases without associated adverse clinical sequelae. There were no major adverse events.
Conclusion: Co-axial sequential injection sacroplasty is a safe and effective technique which allows facilitates controlled delivery of cement. Improved control of cement delivery, including around high-risk structures for cement leakage, offers a potential safety advantage over conventional sacroplasty techniques. Further research comparing technical and clinical outcomes to conventional techniques is warranted.
Keywords: Percutaneous sacroplasty; cement leakage; co-axial sacroplasty; sacral insufficiency fractures; sequential injection.
Figures
References
-
- Kortman K, Ortiz O, Miller T, et al. Multicenter study to assess the efficacy and safety of sacroplasty in patients with osteoporotic sacral insufficiency fractures or pathologic sacral lesions. J NeuroIntervent Surg 2013; 5: 461–466. - PubMed
-
- Frey ME, DePalma MJ, Cifu DX, et al. Percutaneous sacroplasty for osteoporotic sacral insufficiency fractures: a prospective, multicenter, observational pilot study. Spine J 2008; 8: 367–373. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
