

Evaluating the cost-effectiveness of polygenic risk score-stratified screening for abdominal aortic aneurysm
- PMID: 39277617
- PMCID: PMC11401842
- DOI: 10.1038/s41467-024-52452-w
Evaluating the cost-effectiveness of polygenic risk score-stratified screening for abdominal aortic aneurysm
Abstract
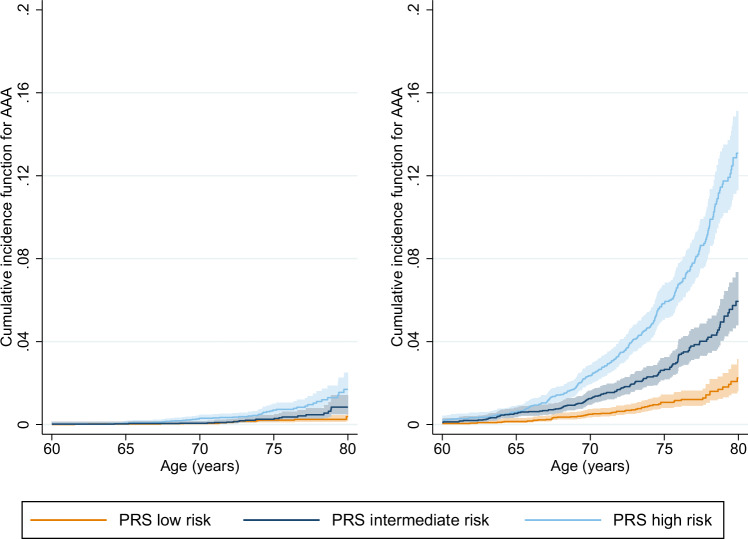
As the heritability of abdominal aortic aneurysm (AAA) is high and AAA partially shares genetic architecture with other cardiovascular diseases, genetic information could help inform AAA screening strategies. Exploiting pleiotropy and meta-analysing summary data from large studies, we construct a polygenic risk score (PRS) for AAA. Leveraging related traits improves PRS performance (R2) by 22.7%, relative to using AAA alone. Compared with the low PRS tertile, intermediate and high tertiles have hazard ratios for AAA of 2.13 (95%CI 1.61, 2.82) and 3.70 (95%CI 2.86, 4.80) respectively, adjusted for clinical risk factors. Using simulation modelling, we compare PRS- and smoking-stratified screening with inviting men at age 65 and not inviting women (current UK strategy). In a futuristic scenario where genomic information is available, our modelling suggests inviting male current smokers with high PRS earlier than 65 and screening female smokers with high/intermediate PRS at 65 and 70 respectively, may improve cost-effectiveness.
© 2024. The Author(s).
Conflict of interest statement
J.D. serves on scientific advisory boards for AstraZeneca, Novartis, and UK Biobank, and has received multiple grants from academic, charitable and industry sources outside of the submitted work. M.I. is a trustee of the Public Health Genomics (PHG) Foundation, a member of the Scientific Advisory Board of Open Targets, and has research collaborations with AstraZeneca, Nightingale Health and Pfizer which are unrelated to this study. M.J.S. reports full-time employment with AstraZeneca and AstraZeneca stock ownership. S.H. is an employee at Genomics PLC. The other authors declare no competing interests.
Figures


References
-
- Abdominal aortic aneurysm screening. nhs.uk. https://www.nhs.uk/conditions/abdominal-aortic-aneurysm-screening/.
-
- Barton, F. & Ward, S. Deaths registered in England and Wales - Office for National Statistics. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarri... (2023).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
