

Pan-tumor validation of a NGS fraction-based MSI analysis as a predictor of response to Pembrolizumab
- PMID: 39277692
- PMCID: PMC11401835
- DOI: 10.1038/s41698-024-00679-7
Pan-tumor validation of a NGS fraction-based MSI analysis as a predictor of response to Pembrolizumab
Abstract
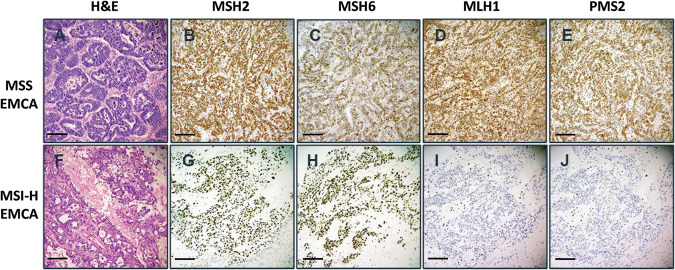
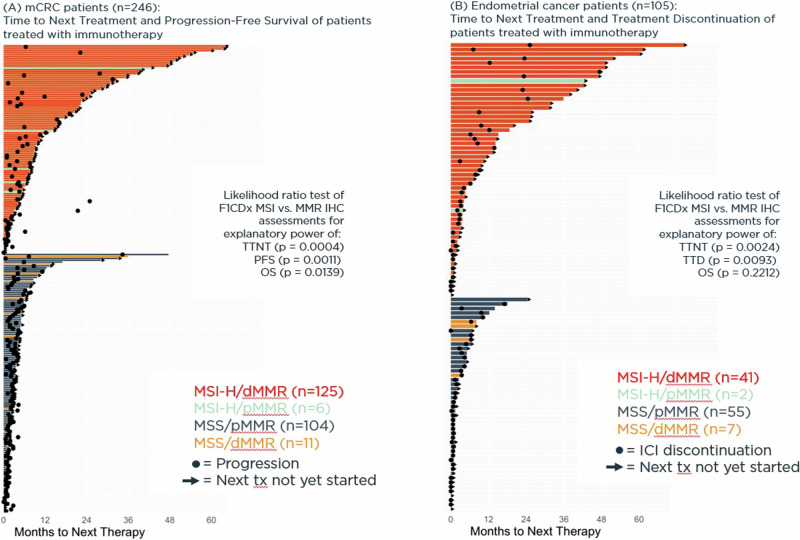
Microsatellite instability high (MSI-H) and mismatch repair deficient (dMMR) tumor status have been demonstrated to predict patient response to immunotherapies. We developed and validated a next-generation sequencing (NGS)-based companion diagnostic (CDx) to detect MSI-H solid tumors via a comprehensive genomic profiling (CGP) assay, FoundationOne®CDx (F1CDx). To determine MSI status, F1CDx calculates the fraction of unstable microsatellite loci across >2000 loci using a fraction-based (FB) analysis. Across solid tumor types, F1CDx demonstrated a high analytical concordance with both PCR (n = 264) and IHC (n = 279) with an overall percent agreement (OPA) of 97.7% and 97.8%, respectively. As part of a retrospective bridging clinical study from KEYNOTE-158 Cohort K and KEYNOTE-164, patients with MSI-H tumors as determined by F1CDx demonstrated an objective response rate (ORR) of 43.0% to pembrolizumab. In real-world cancer patients from a deidentified clinicogenomic database, F1CDx was at least equivalent in assessing clinical outcome following immunotherapy compared with MMR IHC. Demonstrated analytical and clinical performance of F1CDx led to the pan-tumor FDA approval in 2022 of F1CDx to identify MSI-H solid tumor patients for treatment with pembrolizumab. F1CDx is an accurate, reliable, and FDA-approved method for the identification of MSI-H tumors for treatment with pembrolizumab.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: D.I.L., J.C.F.Q., N.D., M.C.H., D.L.S., L.A.A., J.L., D.A.M., B.D., S.L., N.R.P., R.P.G., J.A.E., J.S.R., V.P., and R.S.P.H. are employed by Foundation Medicine, Inc., a wholly-owned subsidiary of Roche, and are stockholders of Roche. L.L., D.L., and A.K.W. are full-time employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and hold stock and/or restricted stock units in Merck & Co., Inc., Rahway, NJ, USA.
Figures

References
-
- Bartley, A. N. et al. Mismatch Repair and Microsatellite Instability Testing for Immune Checkpoint Inhibitor Therapy: Guideline From the College of American Pathologists in Collaboration With the Association for Molecular Pathology and Fight Colorectal Cancer. Arch. Pathol. Lab Med146, 1194–1210 (2022). 10.5858/arpa.2021-0632-CP - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
