

Association between systemic immune inflammation index and short term prognosis of acute on chronic liver failure
- PMID: 39278977
- PMCID: PMC11402960
- DOI: 10.1038/s41598-024-72447-3
Association between systemic immune inflammation index and short term prognosis of acute on chronic liver failure
Abstract
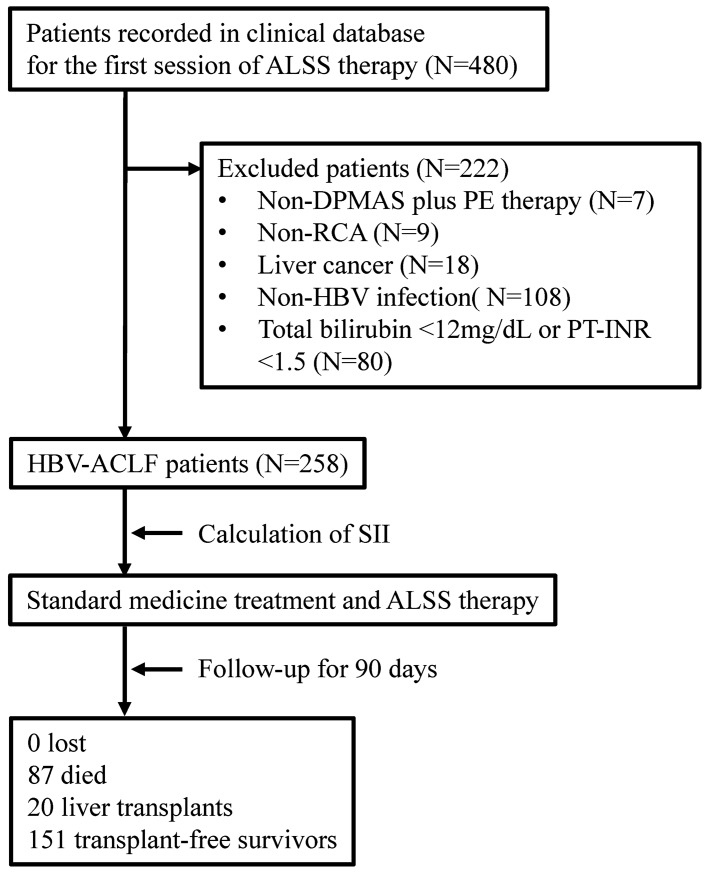
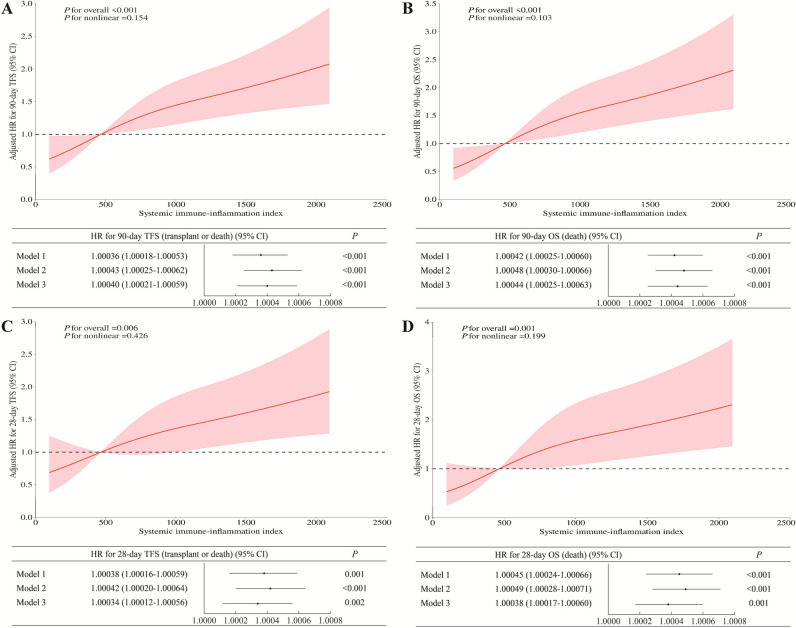
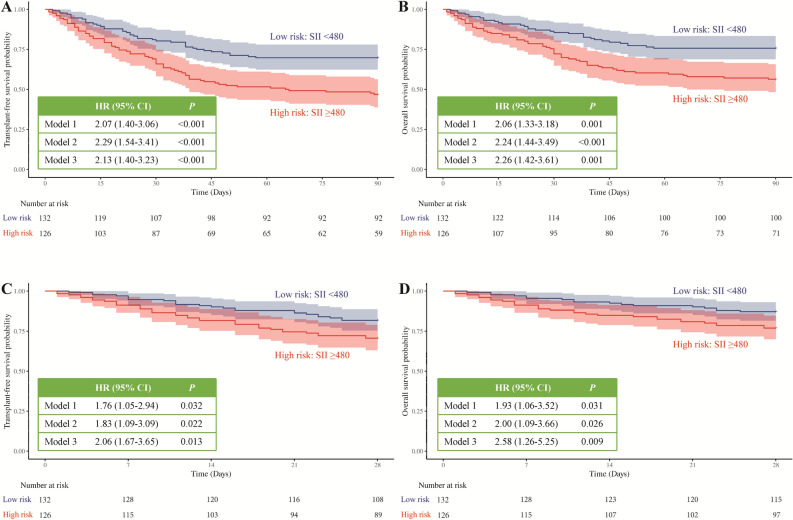
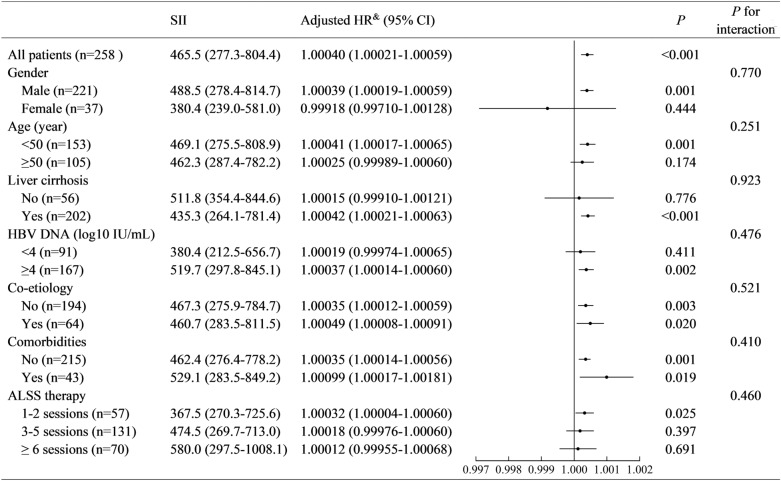
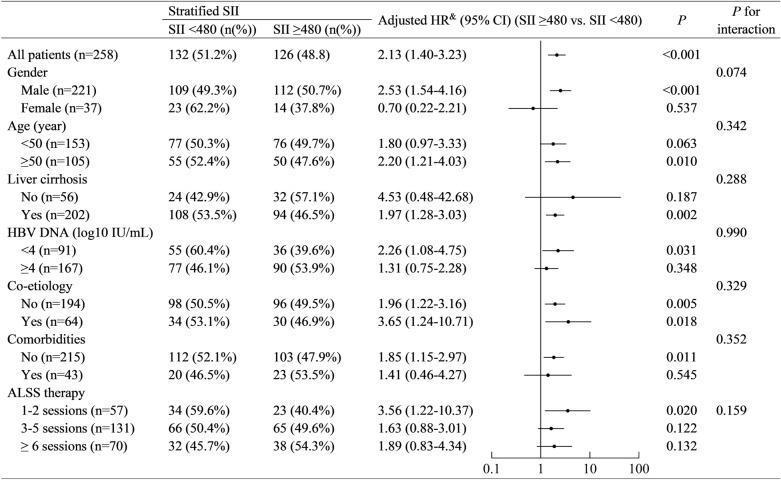
The systemic immune-inflammatory index (SII) has been identified as an independent prognostic factor for multiple diseases. However, the impact of SII on outcome of acute-on-chronic liver failure (ACLF) is scant. A retrospective study enrolled patients with ACLF treated with artificial liver support system. Restricted cubic spline (RCS) (knots at the 10th, 50th, and 90th percentiles) and Cox proportional hazards models were applied to investigate the relationship between SII and 90-day transplant-free survival and overall survival in patients with ACLF. A total of 258 patients with ACLF were included. The 90-day transplant-free survival rate and overall survival rate were 58.5% and 66.3%. The SII was 465.5 (277.3-804.4). Adjusted RCS models showed linear exposure-response relationship between SII and 90-day transplant-free survival (P for overall < 0.001, P for nonlinear = 0.154) and 90-day overall survival (P for overall < 0.001, P for nonlinear = 0.103), and adjusted Cox models confirmed the positive relationship. Compared with patients with SII < 480, patients with ≥ 480 had more serious condition, lower 90-day transplant-free survival rate (46.8% vs. 69.7%, adjusted HR (95% CI) for transplant or death: 2.13 (1.40-3.23), P < 0.001), and lower 90-day overall survival rate (56.3% vs. 75.8%; adjusted HR (95% CI) for death: 2.26 (1.42-3.61), P = 0.001). Stratified Cox models suggested no potential modifiers in the relationship between SII and 90-day transplant-free survival. Our findings suggested SII was positively associated with poor short-term prognosis of ACLF.
Keywords: Acute-on-chronic liver failure; Artificial liver support system; Outcome; Risk factor; Systemic immune-inflammation index.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
