

Point-of-Care Ultrasound: A Vital Tool for Anesthesiologists in the Perioperative and Critical Care Settings
- PMID: 39280520
- PMCID: PMC11401632
- DOI: 10.7759/cureus.66908
Point-of-Care Ultrasound: A Vital Tool for Anesthesiologists in the Perioperative and Critical Care Settings
Abstract
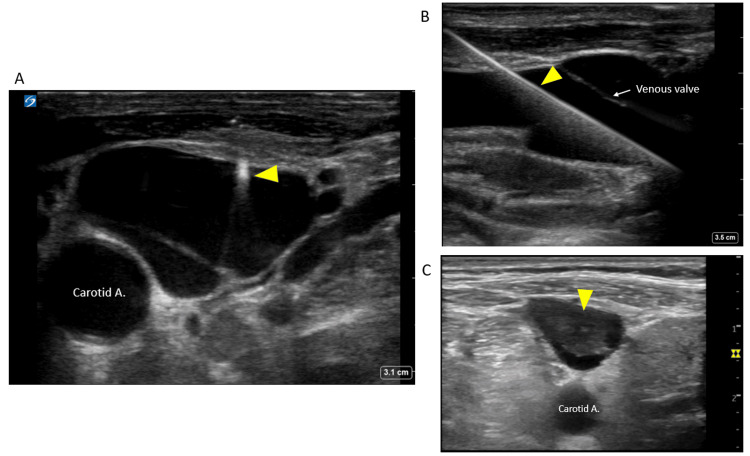
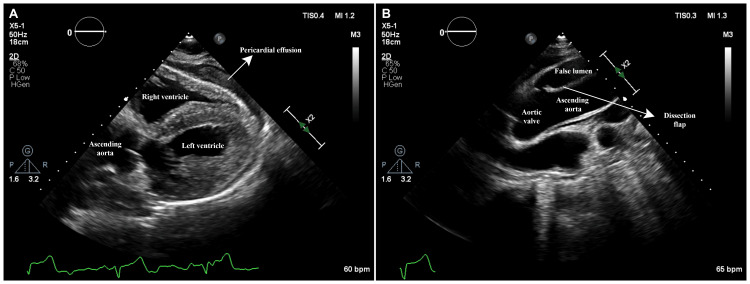
Point-of-care ultrasound (POCUS) is an essential skill in various specialties like anesthesiology, critical care, and emergency medicine. Anesthesiologists utilize POCUS for quick diagnosis and procedural guidance in perioperative and critical care settings. Key applications include vascular ultrasound for challenging venous and arterial catheter placements, gastric ultrasound for aspiration risk assessment, airway ultrasound, diaphragm ultrasound, and lung ultrasound for respiratory assessment. Additional utilities of POCUS can include multi-organ POCUS evaluation for undifferentiated shock or cardiac arrest, ultrasound-guided central neuraxial and peripheral nerve blocks, focused cardiac ultrasound, and novel applications such as venous excess ultrasound. This review highlights these POCUS applications in perioperative and intensive care and summarizes the latest evidence of their accuracy and limitations.
Keywords: airway ultrasound; anaesthesiology; bedside ultrasound; gastric ultrasound; perioperative pocus; pocus (point of care ultrasound).
Copyright © 2024, Dhir et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: Abhilash Koratala declare(s) a grant from KidneyCure and the American Society of Nephrology’s William and Sandra Bennett Clinical Scholars Grant. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures











References
-
- Perioperative point-of-care ultrasound: from concept to application. Ramsingh D, Bronshteyn YS, Haskins S, Zimmerman J. Anesthesiology. 2020;132:908–916. - PubMed
-
- History of emergency and critical care ultrasound: the evolution of a new imaging paradigm. Kendall JL, Hoffenberg SR, Smith RS. Crit Care Med. 2007;35:0–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources