

AI-enhanced diagnostic model for pulmonary nodule classification
- PMID: 39281372
- PMCID: PMC11393475
- DOI: 10.3389/fonc.2024.1417753
AI-enhanced diagnostic model for pulmonary nodule classification
Abstract
Background: The identification of benign and malignant pulmonary nodules (BPN and MPN) can significantly reduce mortality. However, a reliable and validated diagnostic model for clinical decision-making is still lacking.
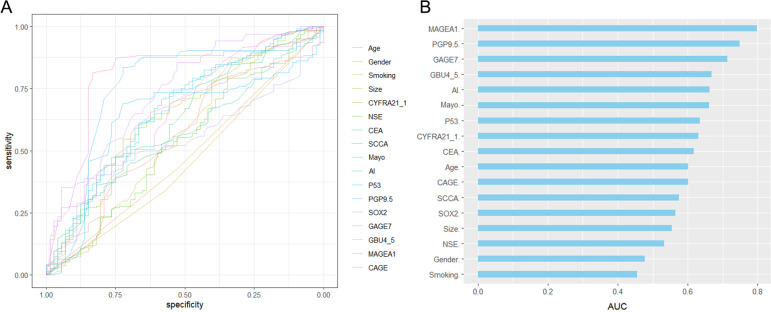
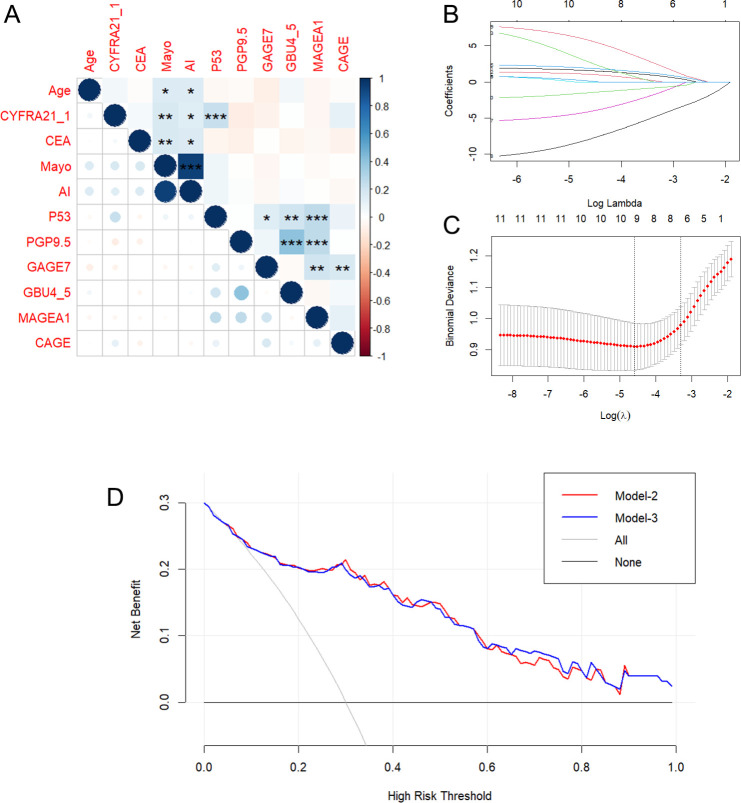
Methods: Enzyme-linked immunosorbent assay and electro chemiluminescent immunoassay were utilized to determine the serum concentrations of 7AABs (p53, GAGE7, PGP9.5, CAGE, MAGEA1, SOX2, GBU4-5), and 4TTMs (CYFR21, CEA, NSE and SCC) in 260 participants (72 BPNs and 188 early-stage MPNs), respectively. The malignancy probability was calculated using Artificial intelligence pulmonary nodule auxiliary diagnosis system, or Mayo model. Along with age, sex, smoking history and nodule size, 18 variables were enrolled for model development. Baseline comparison, univariate ROC analysis, variable correlation analysis, lasso regression, univariate and stepwise logistic regression, and decision curve analysis (DCA) was used to reduce and screen variables. A nomogram and DCA were built for model construction and clinical use. Training (60%) and validation (40%) cohorts were used to for model validation.
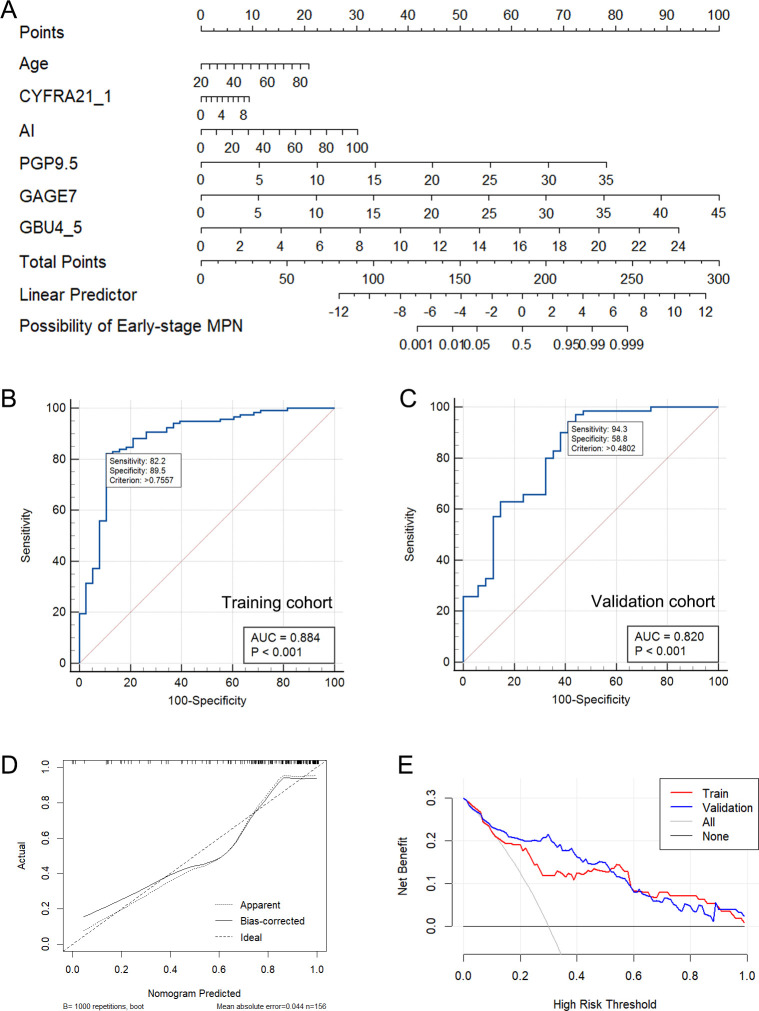
Results: Age, CYFRA21_1, AI, PGP9.5, GAGE7, and GBU4_5 was screened out from 18 variables and utilized to establish the regression model for identifying BPN and early-stage MPN, as well as nomogram and DCA for clinical practical use. The AUC of the nomogram in the training and validation cohorts were 0.884 and 0.820, respectively. Moreover, the calibration curve showed high coherence between the predicted and actual probability.
Conclusion: This diagnostic model and DCA could provide evidence for upgrading or maintaining the current clinical decision based on malignancy probability stratification. It enables low and moderate risk or ambiguous patients to benefit from more precise clinical decision stratification, more timely detection of malignant nodules, and early treatment.
Keywords: DCA; diagnostic model; lung cancer; nomogram; pulmonary nodule.
Copyright © 2024 Chen, Ming, Huang, Wei, Wu, Zhou and Ling.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Clinical value of tumor-associated autoantibodies in diagnosis of early non-small cell lung cancer].Zhonghua Yu Fang Yi Xue Za Zhi. 2021 Dec 6;55(12):1426-1434. doi: 10.3760/cma.j.cn112150-20210511-00461. Zhonghua Yu Fang Yi Xue Za Zhi. 2021. PMID: 34963239 Chinese.
-
[Evaluation of the application value of seven tumor-associated autoantibodies in non-small cell lung cancer based on machine learning algorithms].Zhonghua Yu Fang Yi Xue Za Zhi. 2023 Nov 6;57(11):1827-1838. doi: 10.3760/cma.j.cn112150-20221111-01099. Zhonghua Yu Fang Yi Xue Za Zhi. 2023. PMID: 38008573 Chinese.
-
Establishment and verification of a prediction model based on clinical characteristics and computed tomography radiomics parameters for distinguishing benign and malignant pulmonary nodules.J Thorac Dis. 2024 Mar 29;16(3):1984-1995. doi: 10.21037/jtd-23-1400. Epub 2024 Mar 18. J Thorac Dis. 2024. PMID: 38617763 Free PMC article.
-
Development and validation of a prediction model for malignant pulmonary nodules: A cohort study.Medicine (Baltimore). 2021 Dec 23;100(51):e28110. doi: 10.1097/MD.0000000000028110. Medicine (Baltimore). 2021. PMID: 34941053 Free PMC article.
-
Classification of solid pulmonary nodules using a machine-learning nomogram based on 18F-FDG PET/CT radiomics integrated clinicobiological features.Ann Transl Med. 2022 Dec;10(23):1265. doi: 10.21037/atm-22-2647. Ann Transl Med. 2022. PMID: 36618813 Free PMC article.
Cited by
-
Differential Radiomics-Based Signature Predicts Lung Cancer Risk Accounting for Imaging Parameters in NLST Cohort.Cancer Med. 2024 Oct;13(20):e70359. doi: 10.1002/cam4.70359. Cancer Med. 2024. PMID: 39463128 Free PMC article.
References
-
- SEER*Explorer: An interactive website for SEER cancer statistics. Surveillance Research Program . Explorer, S. E. E. R. An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute.[Cited 2021 April 15]. (2023). Available at: https://seer.cancer.gov/statistics-network/explorer/.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous