Breathing motion compensation in chest tomosynthesis: evaluation of the effect on image quality and presence of artifacts
- PMID: 39281664
- PMCID: PMC11399550
- DOI: 10.1117/1.JMI.12.S1.S13004
Breathing motion compensation in chest tomosynthesis: evaluation of the effect on image quality and presence of artifacts
Abstract
Purpose: Chest tomosynthesis (CTS) has a relatively longer acquisition time compared with chest X-ray, which may increase the risk of motion artifacts in the reconstructed images. Motion artifacts induced by breathing motion adversely impact the image quality. This study aims to reduce these artifacts by excluding projection images identified with breathing motion prior to the reconstruction of section images and to assess if motion compensation improves overall image quality.
Approach: In this study, 2969 CTS examinations were analyzed to identify examinations where breathing motion has occurred using a method based on localizing the diaphragm border in each of the projection images. A trajectory over diaphragm positions was estimated from a second-order polynomial curve fit, and projection images where the diaphragm border deviated from the trajectory were removed before reconstruction. The image quality between motion-compensated and uncompensated examinations was evaluated using the image quality criteria for anatomical structures and image artifacts in a visual grading characteristic (VGC) study. The resulting rating data were statistically analyzed using the software VGC analyzer.
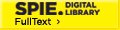
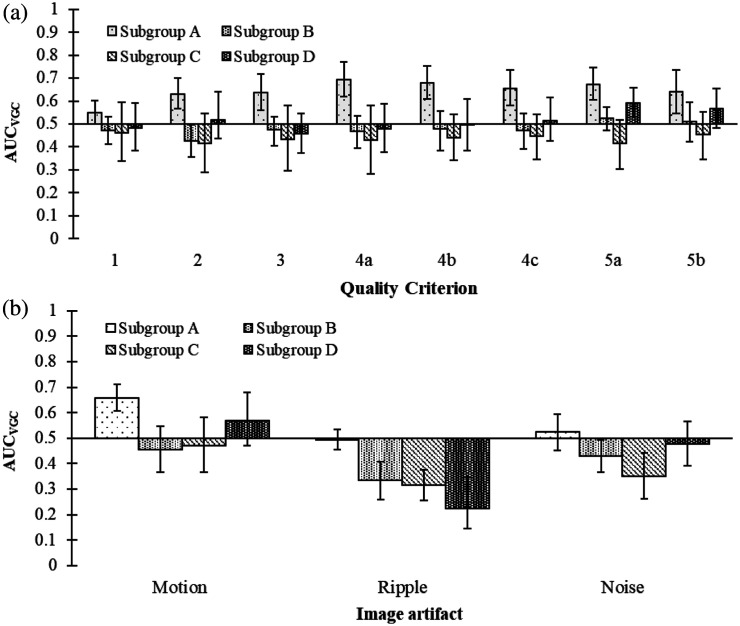
Results: A total of 58 examinations were included in this study with breathing motion occurring either at the beginning or end ( ) or throughout the entire acquisition ( ). In general, no significant difference in image quality or presence of motion artifacts was shown between the motion-compensated and uncompensated examinations. However, motion compensation significantly improved the image quality and reduced the motion artifacts in cases where motion occurred at the beginning or end. In examinations where motion occurred throughout the acquisition, motion compensation led to a significant increase in ripple artifacts and noise.
Conclusions: Compensation for respiratory motion in CTS by excluding projection images may improve the image quality if the motion occurs mainly at the beginning or end of the examination. However, the disadvantages of excluding projections may outweigh the benefits of motion compensation.
Keywords: breathing motion; chest tomosynthesis; image quality; motion artifacts; motion compensation.
© 2024 The Authors.
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials