

Clostridioides difficile infection: an update
- PMID: 39282548
- PMCID: PMC11392548
- DOI: 10.53854/liim-3203-3
Clostridioides difficile infection: an update
Abstract
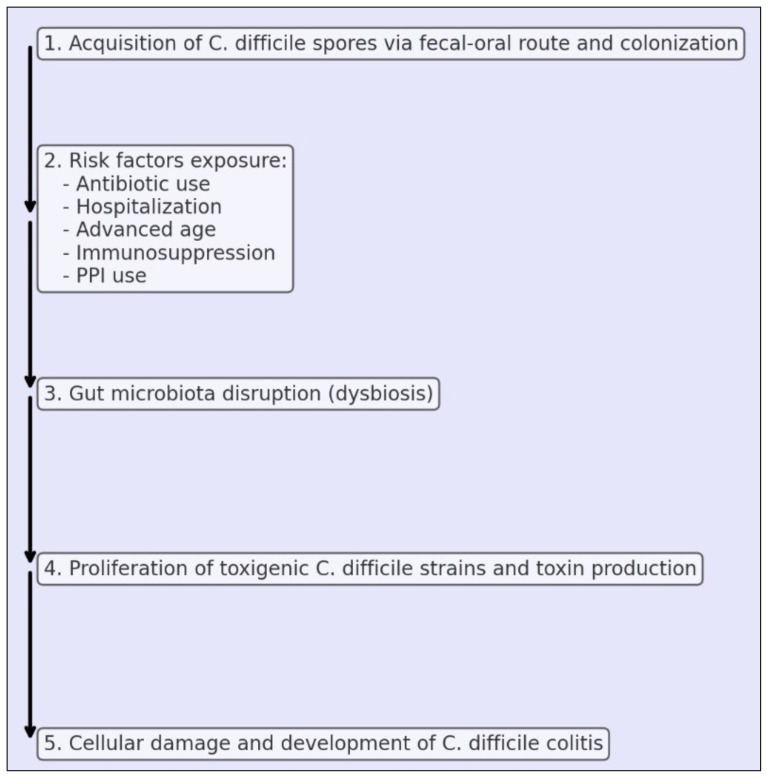
Clostridioides difficile (C. difficile) is a Gram-positive, spore-forming anaerobic bacterium emerged as a leading cause of diarrhea globally. CDI's (Clostridioides difficile infection) impact on healthcare systems is concerning due to high treatment cost and increased hospitalisation time. The incidence of CDI has been influenced by hypervirulent strains such as the 027 ribotype, responsible for significant outbreaks in North America and Europe. CDI's epidemiology has evolved, showing increased community-acquired cases alongside traditional hospital-acquired infections. Mortality rates remain high, with recurrent infections further elevating the risk. Transmission of C. difficile primarily occurs via spores, which survive in healthcare settings and play a pivotal role in transmission. Not only health workers, but also the food chain could have a significant impact on the transmission of infection, although no confirmed foodborne cases have been documented. Pathogenicity of C. difficile involves spore germination and toxin production. Toxins A and B can cause cellular damage and inflammatory responses in the host, leading to colitis. Clinical picture can range from mild diarrhea to fulminant colitis with toxic megacolon, and bowel perforation. Risk factors for CDI include antibiotic exposure, advanced age, hospitalization, and use of proton pump inhibitors. Patients who experience abdominal surgery or patients with inflammatory bowel disease (IBD) are particularly susceptible due to their compromised gut microbiota. Management of CDI has evolved, with fidaxomicin emerging as a superior treatment option over vancomycin for initial and recurrent infections due to its reduction of recurrence rate. Faecal microbiota transplantation (FMT) is effective for recurrent CDI, restoring gut eubiosis. Bezlotoxumab, a monoclonal antibody against C. difficile toxin B, has shown promise in reducing recurrence rates. Severe cases of CDI may require surgical intervention, particularly in instances of toxic megacolon or bowel perforation. In conclusion, CDI remains a significant clinical entity. Further research are needed to improve patients' outcome and reduce the burden on healthcare systems.
Keywords: Clostridioides difficile; bezlotoxumab; fidaxomicin.
Figures
References
-
- European Centre for Disease Prevention and Control. European Surveillance of Clostridioides (Clostridium) Difficile Infections. Surveillance Protocol Version 2.4. ECDC; 2019. Dec, - DOI
-
- Viprey VF, Granata G, Vendrik KEW, et al. COMBACTE-CDI Consortium. European Survey on the Current Surveillance Practices, Management Guidelines, Treatment Pathways and Heterogeneity of Testing of Clostridioides difficile, 2018–2019: Results from The Combatting Bacterial Resistance in Europe CDI (COMBACTE-CDI) J Hosp Infect. 2023;131:213–220. - PubMed
-
- Granata G, Cataldo MA, D’arezzo S, et al. Clostridium difficile infection underdiagnosis in Italy: do we know the true magnitude of the problem? A prospective cohort study. Int J Infect Dis. 2018;73:35–40.
-
- Bertolino L, Patauner F, Gagliardi M, et al. Diagnostic and infection control strategies for Clostridioides difficile infections in a setting of high antimicrobial resistance prevalence. Infez Med. 2021;29(1):70–78. - PubMed
Publication types
LinkOut - more resources
Full Text Sources