

Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors
- PMID: 39282913
- PMCID: PMC11821447
- DOI: 10.1056/NEJMoa2403991
Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors
Abstract
Background: Treatment options for patients with advanced neuroendocrine tumors are limited. The efficacy of cabozantinib in the treatment of previously treated, progressive extrapancreatic or pancreatic neuroendocrine tumors is unclear.
Methods: We enrolled two independent cohorts of patients - those with extrapancreatic neuroendocrine tumors and those with pancreatic neuroendocrine tumors - who had received peptide receptor radionuclide therapy or targeted therapy or both. Patients were randomly assigned in a 2:1 ratio to receive cabozantinib at a dose of 60 mg daily or placebo. The primary end point was progression-free survival as assessed by blinded independent central review. Key secondary end points included objective response, overall survival, and safety.
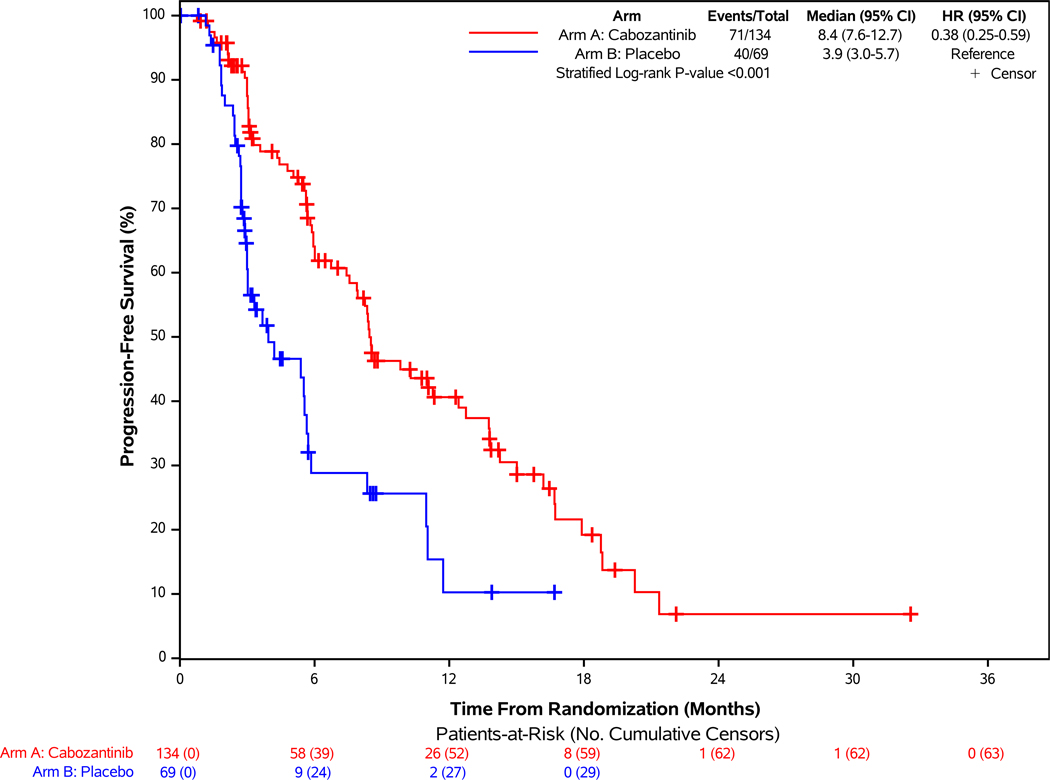
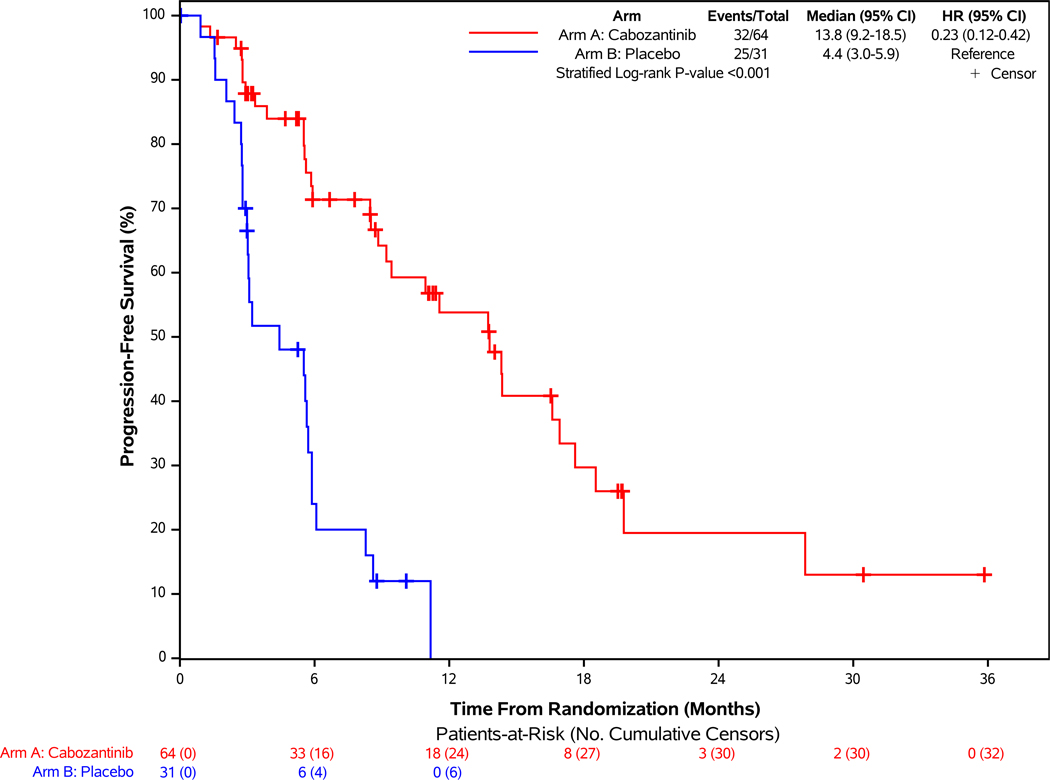
Results: In the cohort of 203 patients with extrapancreatic neuroendocrine tumors, the median progression-free survival with cabozantinib was 8.4 months, as compared with 3.9 months with placebo (stratified hazard ratio for progression or death, 0.38; 95% confidence interval [CI], 0.25 to 0.59; P<0.001). In the cohort of 95 patients with pancreatic neuroendocrine tumors, the median progression-free survival with cabozantinib was 13.8 months, as compared with 4.4 months with placebo (stratified hazard ratio, 0.23; 95% CI, 0.12 to 0.42; P<0.001). The incidence of confirmed objective response with cabozantinib was 5% and 19% among patients with extrapancreatic and pancreatic neuroendocrine tumors, respectively, as compared with 0% with placebo. Grade 3 or higher adverse events were noted in 62 to 65% of the patients treated with cabozantinib, as compared with 23 to 27% of the patients who received placebo. Common treatment-related adverse events of grade 3 or higher included hypertension, fatigue, diarrhea, and thromboembolic events.
Conclusions: Cabozantinib, as compared with placebo, significantly improved progression-free survival in patients with previously treated, progressive advanced extrapancreatic or pancreatic neuroendocrine tumors. Adverse events were consistent with the known safety profile of cabozantinib. (Funded by the National Cancer Institute and others; CABINET ClinicalTrials.gov number, NCT03375320.).
Copyright © 2024 Massachusetts Medical Society.
Figures

Comment in
-
Cabozantinib in Advanced Neuroendocrine Tumors.N Engl J Med. 2025 May 8;392(18):1869. doi: 10.1056/NEJMc2503524. N Engl J Med. 2025. PMID: 40334169 No abstract available.
-
Cabozantinib in Advanced Neuroendocrine Tumors. Reply.N Engl J Med. 2025 May 8;392(18):1869-1870. doi: 10.1056/NEJMc2503524. N Engl J Med. 2025. PMID: 40334170 No abstract available.
References
-
- Rinke A, Müller HH, Schade-Brittinger C, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009;27(28):4656–63. (In eng). DOI: 10.1200/jco.2009.22.8510. - DOI - PubMed
-
- Brabander T, van der Zwan WA, Teunissen JJM, et al. Long-Term Efficacy, Survival, and Safety of [(177)Lu-DOTA(0),Tyr(3)]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin Cancer Res 2017;23(16):4617–4624. (In eng). DOI: 10.1158/1078-0432.Ccr-16-2743. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UG1 CA233329/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10CA180820/CA/NCI NIH HHS/United States
- U10CA180821 and U10CA180882/CA/NCI NIH HHS/United States
- UG1CA233329, UG1CA233331/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180868/CA/NCI NIH HHS/United States
- U10CA180888/CA/NCI NIH HHS/United States
- UG1 CA233290/CA/NCI NIH HHS/United States
- UG1 CA233331/CA/NCI NIH HHS/United States
- UG1 CA189804/CA/NCI NIH HHS/United States
- UG1 CA189856/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- U10CA180868/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- UG1CA189856, UG1CA232760, UG1CA233180, UG1CA233290/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical