

Vascular cognitive impairment and dementia: Mechanisms, treatment, and future directions
- PMID: 39283037
- PMCID: PMC11490097
- DOI: 10.1177/17474930241279888
Vascular cognitive impairment and dementia: Mechanisms, treatment, and future directions
Abstract
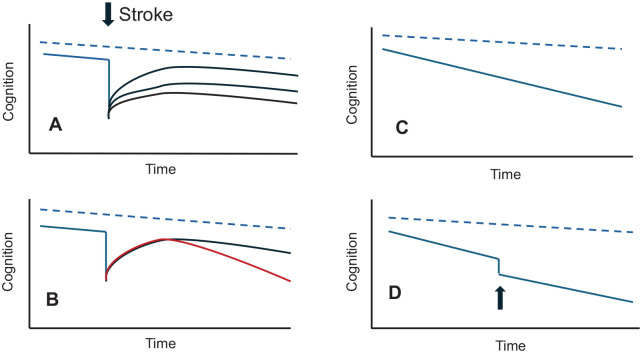
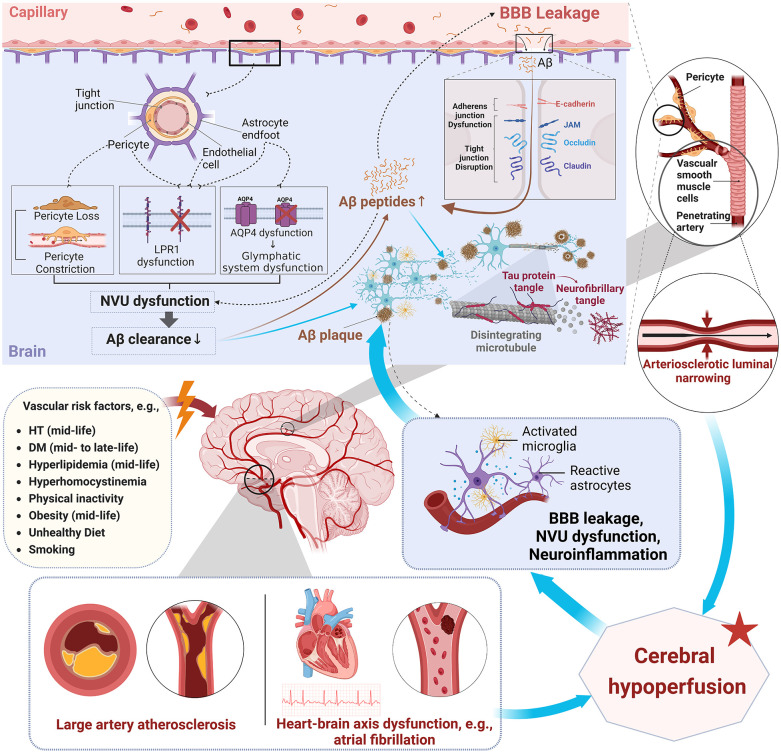
Worldwide, around 50 million people live with dementia, and this number is projected to triple by 2050. It has been estimated that 20% of all dementia cases have a predominant cerebrovascular pathology, while perhaps another 20% of vascular diseases contribute to a mixed dementia picture. Therefore, the vascular contribution to dementia affects 20 million people currently and will increase markedly in the next few decades, particularly in lower- and middle-income countries.In this review, we discuss the mechanisms of vascular cognitive impairment (VCI) and review management. VCI refers to the spectrum of cerebrovascular pathologies that contribute to any degree of cognitive impairment, ranging from subjective cognitive decline, to mild cognitive impairment, to dementia. While acute cognitive decline occurring soon after a stroke is the most recognized form of VCI, chronic cerebrovascular disease, in particular cerebral small-vessel disease, can cause insidious cognitive decline in the absence of stroke. Moreover, cerebrovascular disease not only commonly co-occurs with Alzheimer's disease (AD) and increases the probability that AD pathology will result in clinical dementia, but may also contribute etiologically to the development of AD pathologies.Despite its enormous health and economic impact, VCI has been a neglected research area, with few adequately powered trials of therapies, resulting in few proven treatments. Current management of VCI emphasizes prevention and treatment of stroke and vascular risk factors, with most evidence for intensive hypertension control. Reperfusion therapies in acute stroke may attenuate the risk of VCI. Associated behavioral symptoms such as apathy and poststroke emotionalism are common. We also highlight novel treatment strategies that will hopefully lead to new disease course-modifying therapies. Finally, we highlight the importance of including cognitive endpoints in large cardiovascular prevention trials and the need for an increased research focus and funding for this important area.
Keywords: Alzheimer’s disease; Vascular cognitive impairment; dementia; small-vessel disease; stroke; vascular risk factors.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Patterson C. World Alzheimer report 2018, 2018, https://www.alzint.org/resource/world-alzheimer-report-2018/
-
- Rost NS, Brodtmann A, Pase MP, et al.. Post-stroke cognitive impairment and dementia. Circ Res 2022; 130: 1252–1271. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
