

Characterizing the Use of Time-Limited Trials in Patients With Acute Respiratory Failure: A Prospective, Single-Center Observational Study
- PMID: 39283228
- PMCID: PMC11407817
- DOI: 10.1097/CCE.0000000000001148
Characterizing the Use of Time-Limited Trials in Patients With Acute Respiratory Failure: A Prospective, Single-Center Observational Study
Abstract
Importance: A time-limited trial (TLT) is a collaborative plan among clinicians, patients, and families to use life-sustaining therapy for a defined duration, after which the patient's response informs whether to continue care directed toward recovery or shift the focus toward comfort. TLTs are a promising approach to help navigate uncertainty in critical illness, yet little is known about their current use.
Objectives: To characterize TLT use in patients with acute respiratory failure (ARF).
Design, setting, and participants: Prospective 12-month observational cohort study at an U.S. academic medical center of adult ICU patients with ARF receiving invasive mechanical ventilation for greater than or equal to 48 hours.
Main outcomes and measures: Primary exposure was TLT participation, identified by patients' ICU physician. Patient characteristics, care delivery elements, and hospital outcomes were extracted from the electronic medical record.
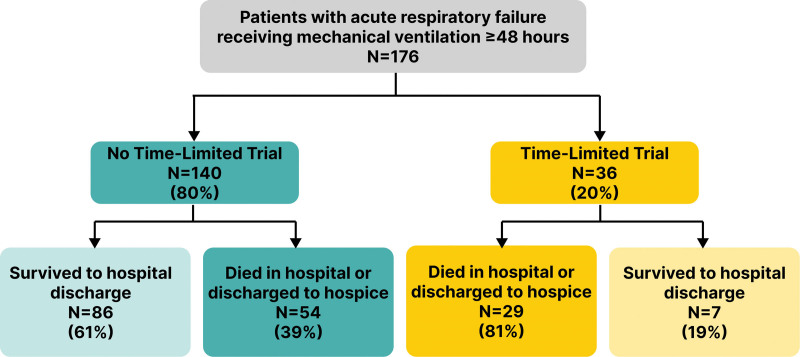
Results: Among 176 eligible patients, 36 (20.5%) participated in a TLT. Among 18 ICU attending physicians, nine (50%) participated in greater than or equal to 1 TLT (frequency 0-39% of patients cared for). Median TLT duration was 3.0 days (interquartile range [IQR], 3.0-4.5 d). TLT patients had a higher mean age (67.4 yr [sd, 12.0 yr] vs. 60.0 yr [sd, 16.0 yr]; p < 0.01), higher Charlson Comorbidity Index (5.1 [sd, 2.2] vs. 3.8 [sd, 2.6]; p < 0.01), and similar Sequential Organ Failure Assessment score (9.6 [sd, 3.3] vs. 9.5 [sd, 3.7]; p = 0.93), compared with non-TLT patients. TLT patients were more likely to die or be discharged to hospice (80.6% vs. 42.1%; p < 0.05) and had shorter ICU length of stay (median, 5.7 d [IQR, 4.0-9.0 d] vs. 10.3 d [IQR, 5.5-14.5 d]; p < 0.01).
Conclusions and relevance: In this study, approximately one in five patients with ARF participated in a TLT. Our findings suggest TLTs are used primarily in patients near end of life but with substantial physician variation, highlighting a need for evidence to guide optimal use.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Kruser was supported, in part, by National Institutes of Health/National Heart, Lung, and Blood Institute grant K23HL146890 and R01HL168474. Dr. Kruser’s spouse receives honoraria for lectures and speakers bureaus from Astra Zeneca. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures


References
-
- Meadow W, Pohlman A, Frain L, et al. : Power and limitations of daily prognostications of death in the medical intensive care unit. Crit Care Med 2011; 39:474–479 - PubMed
-
- Meadow W, Pohlman A, Reynolds D, et al. : Power and limitations of daily prognostications of death in the medical ICU for outcomes in the following 6 months. Crit Care Med 2014; 42:2387–2392 - PubMed
-
- Quill TE, Holloway R: Time-limited trials near the end of life. JAMA 2011; 306:1483–1484 - PubMed
-
- Vink EE, Azoulay E, Caplan A, et al. : Time-limited trial of intensive care treatment: An overview of current literature. Intensive Care Med 2018; 44:1369–1377 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
