

The Impact of Unrelated Future Medical Costs on Economic Evaluation Outcomes for Different Models of Diabetes
- PMID: 39283475
- PMCID: PMC11470878
- DOI: 10.1007/s40258-024-00914-z
The Impact of Unrelated Future Medical Costs on Economic Evaluation Outcomes for Different Models of Diabetes
Abstract
Objective: This study leveraged data from 11 independent international diabetes models to evaluate the impact of unrelated future medical costs on the outcomes of health economic evaluations in diabetes mellitus.
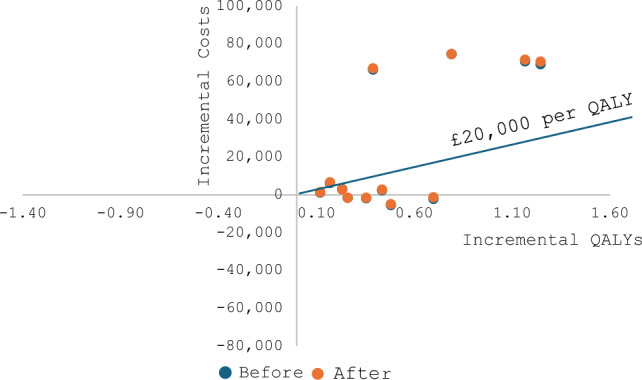
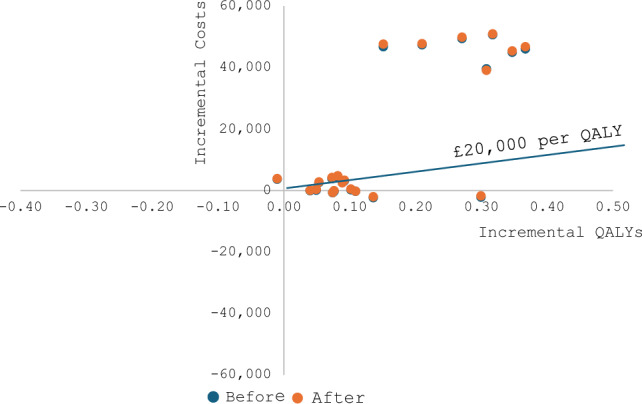
Methods: Eleven models simulated the progression of diabetes and occurrence of its complications in hypothetical cohorts of individuals with type 1 (T1D) or type 2 (T2D) diabetes over the remaining lifetime of the patients to evaluate the cost effectiveness of three hypothetical glucose improvement interventions versus a hypothetical control intervention. All models used the same set of costs associated with diabetes complications and interventions, using a United Kingdom healthcare system perspective. Standard utility/disutility values associated with diabetes-related complications were used. Unrelated future medical costs were assumed equal for all interventions and control arms. The statistical significance of changes on the total lifetime costs, incremental costs and incremental cost-effectiveness ratios (ICERs) before and after adding the unrelated future medical costs were analysed using t-test and summarized in incremental cost-effectiveness diagrams by type of diabetes.
Results: The inclusion of unrelated costs increased mean total lifetime costs substantially. However, there were no significant differences between the mean incremental costs and ICERs before and after adding unrelated future medical costs. Unrelated future medical cost inclusion did not alter the original conclusions of the diabetes modelling evaluations.
Conclusions: For diabetes, with many costly noncommunicable diseases already explicitly modelled as complications, and with many interventions having predominantly an effect on the improvement of quality of life, unrelated future medical costs have a small impact on the outcomes of health economic evaluations.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- Kearns B. The relevance of future, unrelated health costs in economic evaluation in NICE appraisals. In: NICE dsu report. 2020.
-
- Van Baal PHM, Feenstra TL, Hoogenveen RT, Ardine De Wit G, Brouwer WBF. Unrelated medical care in life years gained and the cost utility of primary prevention: in search of a ‘perfect’ cost–utility ratio. Health Econ. 2007;16(4):421–33. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
