

Epidural Analgesia During Labor and Neonatal Hypoxic-Ischemic Encephalopathy
- PMID: 39283635
- PMCID: PMC11406397
- DOI: 10.1001/jamanetworkopen.2024.33730
Epidural Analgesia During Labor and Neonatal Hypoxic-Ischemic Encephalopathy
Abstract
Importance: Epidural analgesia is used by approximately 70% of birthing persons in the US to alleviate labor pain and is a common cause of elevated temperature in the birthing parent during labor, which, in turn, is associated with adverse neonatal outcomes such as hypoxic-ischemic encephalopathy (HIE).
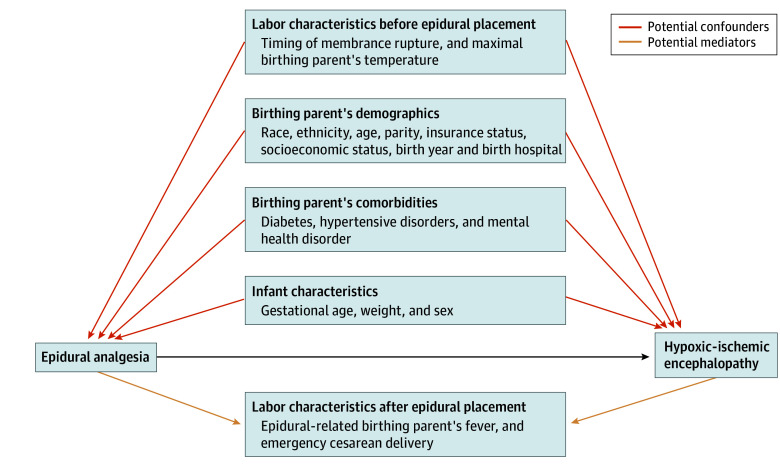
Objective: To determine whether epidural analgesia is associated with increased risk of HIE after adjusting for the birthing person's maximal temperature before epidural placement and for the propensity to get an epidural.
Design, setting, and participants: This retrospective, population-based cohort study was conducted at 15 Kaiser Permanente Northern California hospitals. Participants included singleton neonates born at 35 weeks' or later gestational age between 2012 and 2019. Elective cesarean deliveries and deliveries within 2 hours of hospital admission were excluded. Data analysis was performed from November 2022 to June 2024.
Exposure: The primary exposure was epidural analgesia during labor.
Main outcomes and measures: The primary outcome was HIE, defined as the presence of both neonatal acidosis (ie, pH <7 or base deficit ≥10) and encephalopathy. The presence and timing of epidural analgesia and demographic, pregnancy, and labor characteristics were extracted from electronic medical records. A propensity score for receiving epidural analgesia was created including demographic variables and comorbidities predating epidural placement. Logistic regression was used to evaluate the association between epidural analgesia and HIE, adjusting for maximal birthing parent's temperature before epidural placement and the propensity for receiving an epidural.
Results: Among 233 056 infants born at 35 weeks' or later gestational age by vaginal or unplanned cesarean delivery after at least 2 hours of in-hospital labor, 177 603 (76%) were exposed to epidural analgesia and 439 (0.19%) had HIE. On unadjusted analysis, epidural analgesia was associated with an increased risk of maximal temperature greater than 38 °C during labor (risk ratio [RR], 8.58; 95% CI, 8.06-9.14). Each degree increase in maximal temperature during labor was associated with nearly triple the odds of HIE (odds ratio [OR], 2.82; 95% CI, 2.51-3.17). However, there was no significant association between epidural analgesia and the risk of HIE either on crude (RR, 1.21; 95% CI, 0.96-1.53) or adjusted (adjusted OR, 0.93; 95% CI, 0.73-1.17) analyses.
Conclusions and relevance: In this cohort study including more than 230 000 parent-infant dyads, epidural analgesia was associated with increased maximal temperature during labor, a known risk factor for HIE. However, epidural analgesia was not associated with increased odds of HIE.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
