

Contribution of major histocompatibility complex class II immunostaining in distinguishing idiopathic inflammatory myopathy subgroups: A histopathological cohort study
- PMID: 39283714
- PMCID: PMC11576552
- DOI: 10.1093/jnen/nlae098
Contribution of major histocompatibility complex class II immunostaining in distinguishing idiopathic inflammatory myopathy subgroups: A histopathological cohort study
Abstract
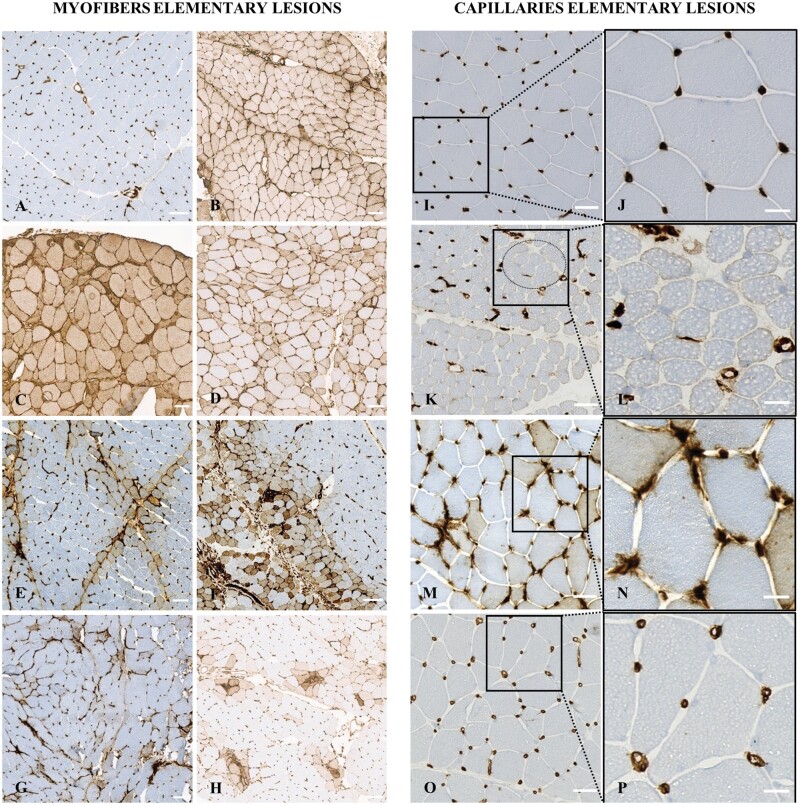
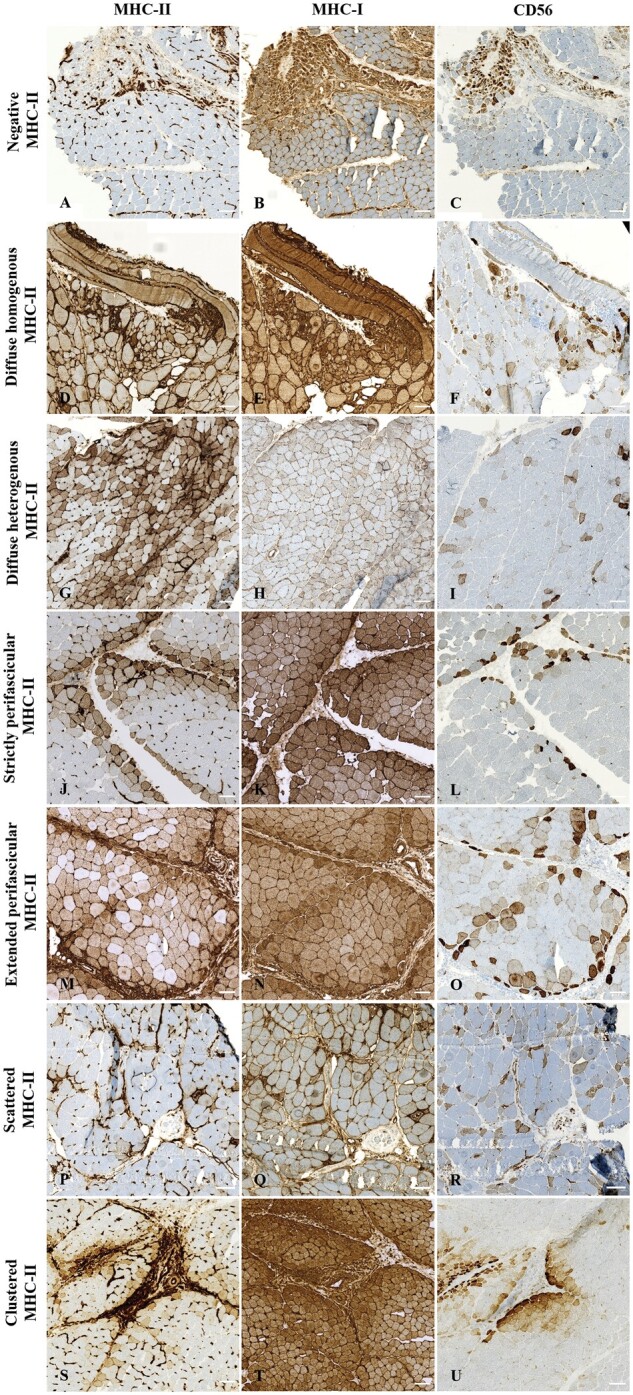
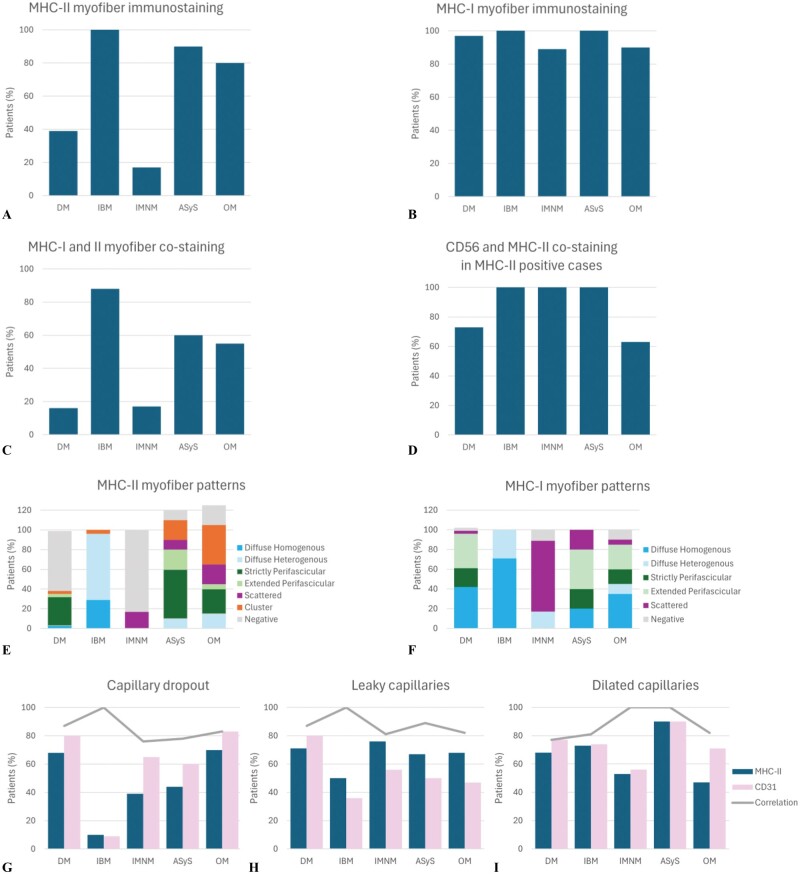
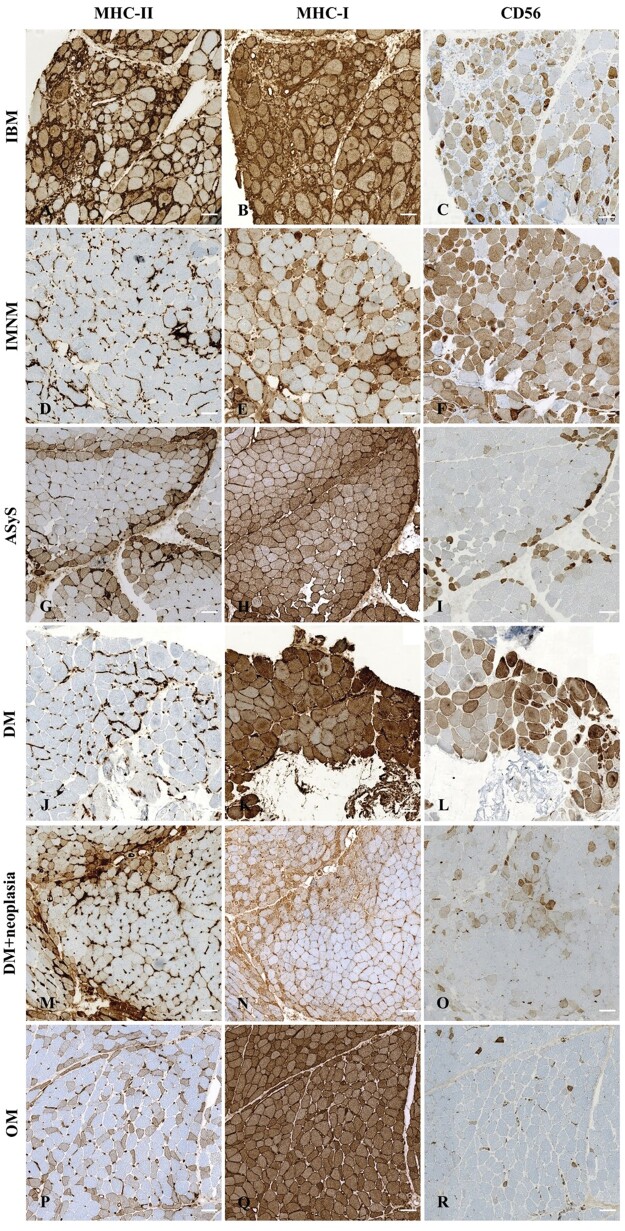
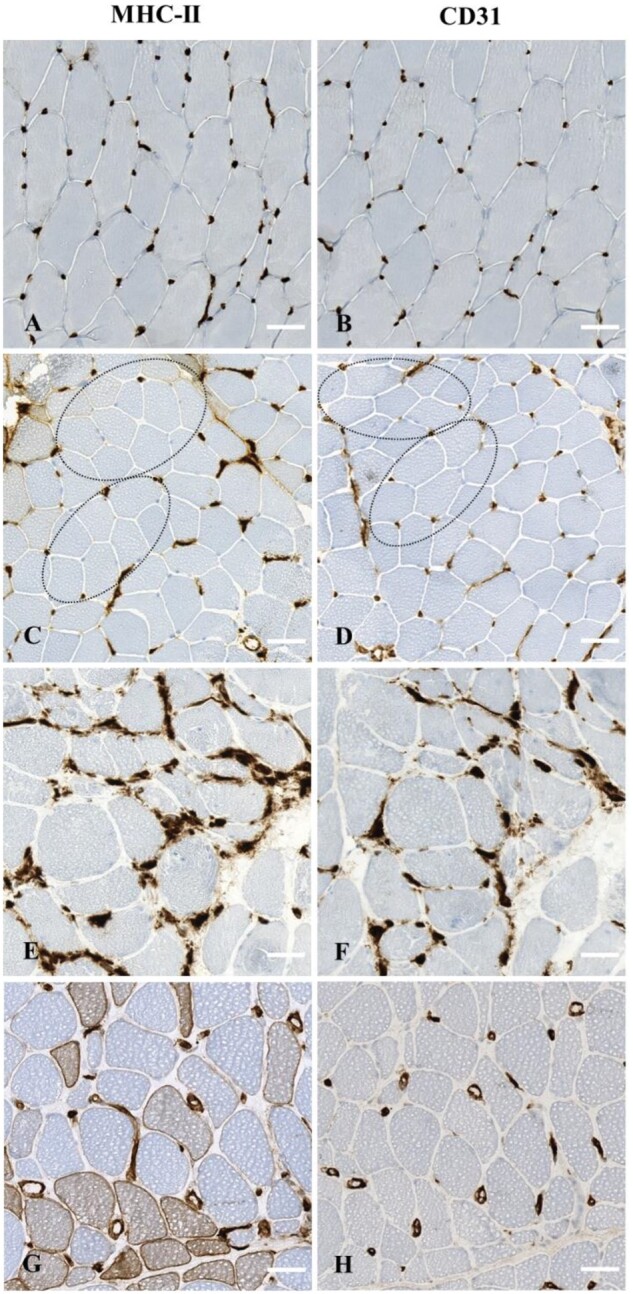
Idiopathic inflammatory myopathies (IIM) are rare, acquired muscle diseases; their diagnosis of is based on clinical, serological, and histological criteria. MHC-I-positive immunostaining, although non-specific, is used as a marker for IIM diagnosis; however, the significance of major histocompatibility complex (MHC)-II immunostaining in IIM remains debated. We investigated patterns of MHC-II immunostaining in myofibers and capillaries in muscle biopsies from 103 patients with dermatomyositis ([DM], n = 31), inclusion body myositis ([IBM], n = 24), anti-synthetase syndrome ([ASyS], n = 10), immune-mediated necrotizing myopathy ([IMNM], n = 18), or overlap myositis ([OM], n = 20). MHC-II immunostaining of myofibers was abnormal in 63/103 of patients (61%) but the patterns differed according to the IIM subgroup. They were diffuse in IBM (96%), negative in IMNM (83%), perifascicular in ASyS (70%), negative (61%) or perifascicular (32%) in DM, and either clustered (40%), perifascicular (30%), or diffuse heterogeneous (15%) in OM. Capillary MHC-II immunostaining also identified quantitative (capillary dropout, n = 47/88, 53%) and qualitative abnormalities, that is, architectural abnormalities, including dilated and leaky capillaries, (n = 79/98, 81%) in all IIM subgroups. Thus, MHC-II myofiber expression patterns allow distinguishing among IIM subgroups. We suggest the addition of MHC-II immunostaining to routine histological panels for IIM diagnosis.
Keywords: capillary; idiopathic inflammatory myopathies; major histocompatibility complex-II; muscle biopsy; myofiber.
© The Author(s) 2024. Published by Oxford University Press on behalf of American Association of Neuropathologists, Inc.
Conflict of interest statement
Authors have no disclosures to declare related to the content of this article.
Figures
References
-
- Meyer A, Meyer N, Schaeffer M, et al. Incidence and prevalence of inflammatory myopathies: a systematic review. Rheumatology (Oxford). 2015;54:50-63. - PubMed
-
- Allenbach Y, Mammen AL, Benveniste O, et al. 224th ENMC International Workshop: clinico-sero-pathological classification of immune-mediated necrotizing myopathies Zandvoort, The Netherlands, 14-16 October 2016. Neuromuscul Disord. 2018;28:87-99. - PubMed
-
- Mammen AL, Allenbach Y, Stenzel W, et al. ENMC 239th Workshop Study Group. 239th ENMC International Workshop: classification of dermatomyositis, Amsterdam, the Netherlands, 14-16 December 2018. Neuromuscul Disord. 2020;30:70-92. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
