

The observation that older men suffer from hip fracture at DXA T-scores higher than older women and a proposal of a new low BMD category, osteofrailia, for predicting fracture risk in older men
- PMID: 39284928
- PMCID: PMC11953210
- DOI: 10.1007/s00256-024-04793-2
The observation that older men suffer from hip fracture at DXA T-scores higher than older women and a proposal of a new low BMD category, osteofrailia, for predicting fracture risk in older men
Abstract
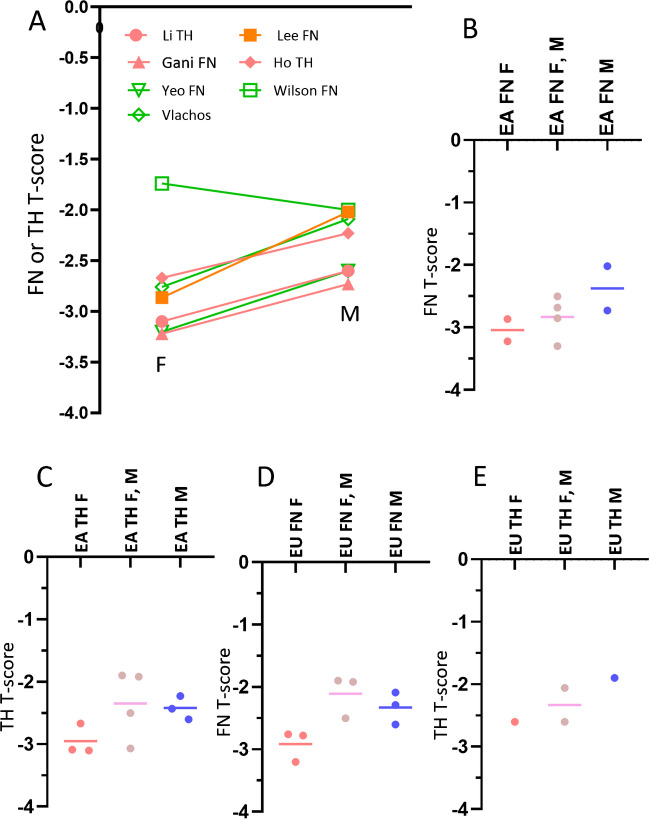
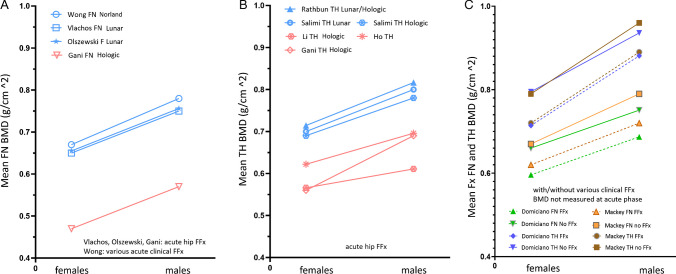
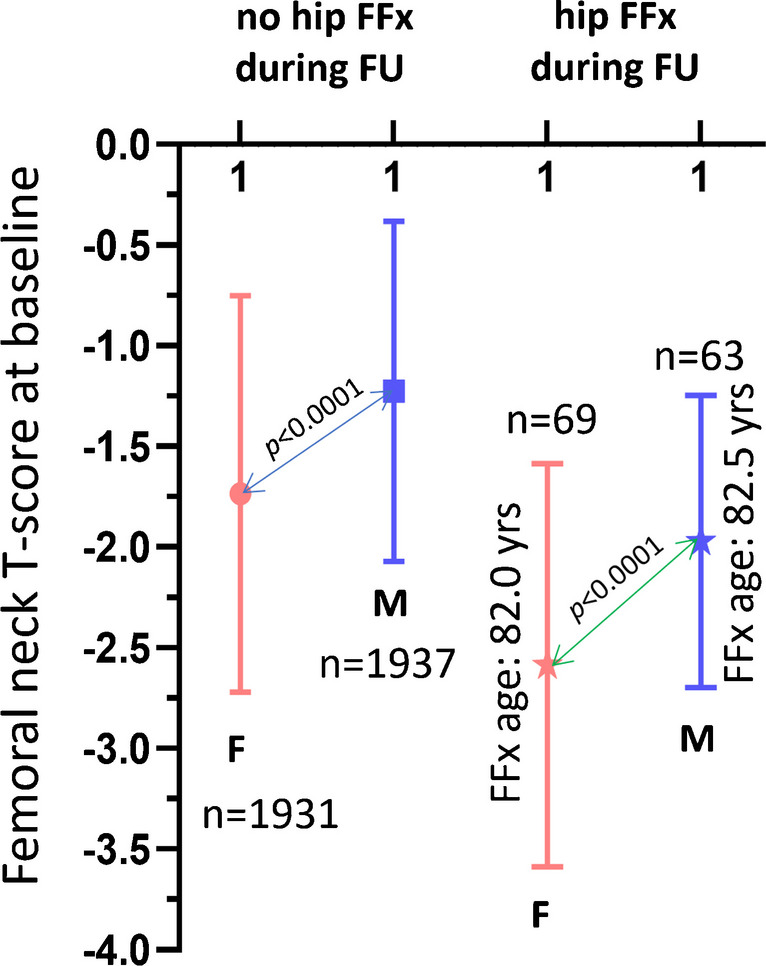
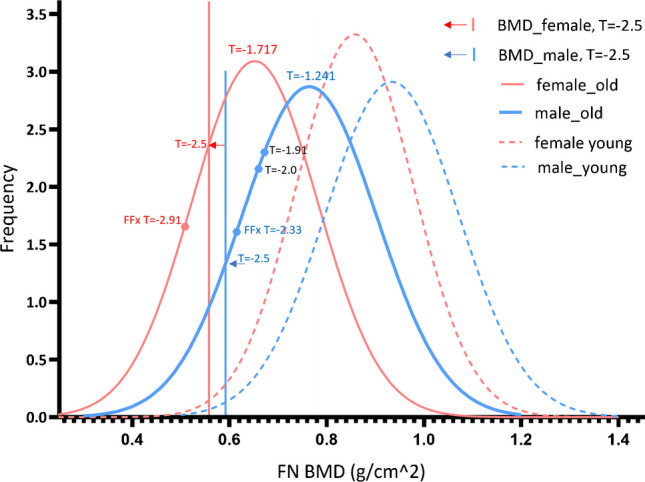
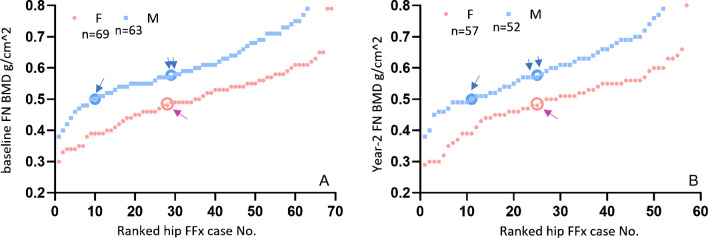
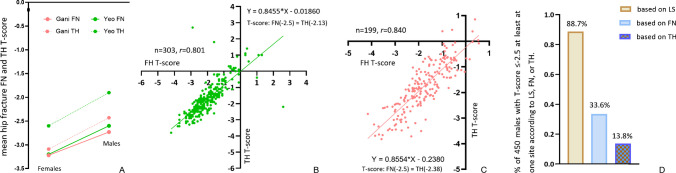
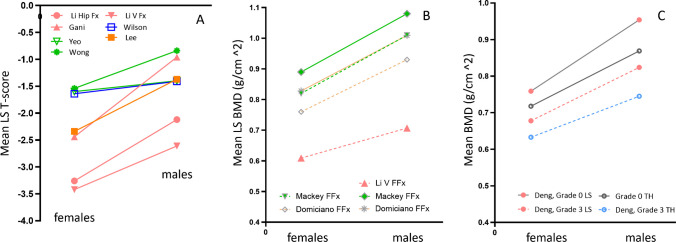
The clinical significance of osteoporosis lies in the occurrence of fragility fractures (FFx), and the most relevant fracture site is the hip. The T-score is defined as follows: (BMDpatient-BMDyoung adult mean)/SDyoung adult population, where BMD is bone mineral density and SD is the standard deviation. When the femoral neck (FN) is measured in adult Caucasian women, a cutpoint value of patient BMD of 2.5 SD below the young adult mean BMD results in a prevalence the same as the lifetime risk of hip FFx for Caucasian women. The FN T-score criterion for classifying osteoporosis in older Caucasian men has been provisionally recommended to be - 2.5, but debates remain. Based on a systematic literature review, we noted that older men suffer from hip FFx at a FN T-score approximately 0.5-0.6 higher than older women. While the mean hip FFx FN T-score of around - 2.9 for women lies below - 2.5, the mean hip FF FN T-score of around - 2.33 for men lies above - 2.5. This is likely associated with that older male populations have a higher mean T-score than older female populations. We propose a new category of low BMD status, osteofrailia, for older Caucasian men with T-score ≤ - 2 (T-score ≤ - 2.1 for older Chinese men) who are likely to suffer from hip FFx. The group with T-score ≤ - 2 for older Caucasian men is comparable in prevalence to the group with T-score ≤ - 2.5 for older Caucasian women. However, older men in such category on average have only half the FFx risk as that of older women with osteoporotic T-score.
Keywords: T-score; Bone mineral density (BMD); Males; Osteoporosis; Reference database.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: A. G. is a shareholder of BICL and LLC and consultant to Pfizer, ICM, TrialSpark, TissueGene, Coval, Medipost, and Novartis. Other authors declare no competing interests.
Figures
References
-
- World Health Organization. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis : report of a WHO study group [meeting held in Rome from 22 to 25 June 1992]. 1994. Available online: https://apps.who.int/iris/handle/10665/39142. Accessed 20 Aug 2023. - PubMed
-
- Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R. Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int. 1998;8:468–89. - PubMed
-
- Wáng YXJ. Estimation of osteoporosis prevalence among a population is reasonable only after the concerned reference bone mineral density database and cutpoint T-score have been validated. Osteoporos Int. 2023;34:417–8. - PubMed
-
- Kanis JA, Johnell O, Oden A, De Laet C, Mellstrom D. Diagnosis of osteoporosis and fracture threshold in men. Calcif Tissue Int. 2001;69:218–21. - PubMed
-
- de Laet CE, van der Klift M, Hofman A, Pols HA. Osteoporosis in men and women: a story about bone mineral density thresholds and hip fracture risk. J Bone Miner Res. 2002;17:2231–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
