

A Framework for the Use and Likelihood of Regulatory Acceptance of Single-Arm Trials
- PMID: 39285061
- PMCID: PMC11530569
- DOI: 10.1007/s43441-024-00693-8
A Framework for the Use and Likelihood of Regulatory Acceptance of Single-Arm Trials
Abstract
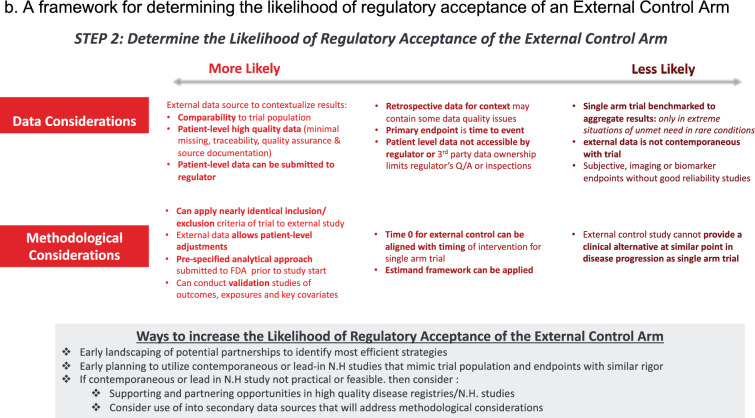
Background: Single-arm clinical trials (SAT) are common in drug and biologic submissions for rare or life-threatening conditions, especially when no therapeutic options exist. External control arms (ECAs) improve interpretation of SATs but pose methodological and regulatory challenges.
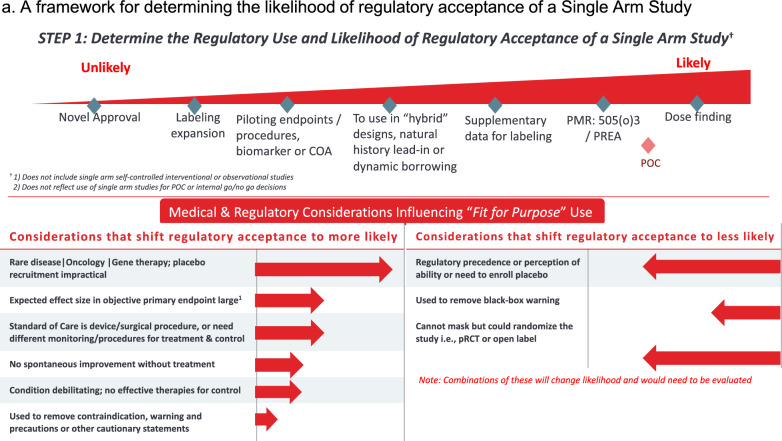
Objective: Through narrative reviews and expert input, we developed a framework for considerations that might influence regulatory use and likelihood of regulatory acceptance of an SAT, identifying non-oncology first indication approvals as an area of interest. We systematically analyzed FDA and EMA approvals using SATs as pivotal evidence. The framework guided outcome abstraction on regulatory responses.
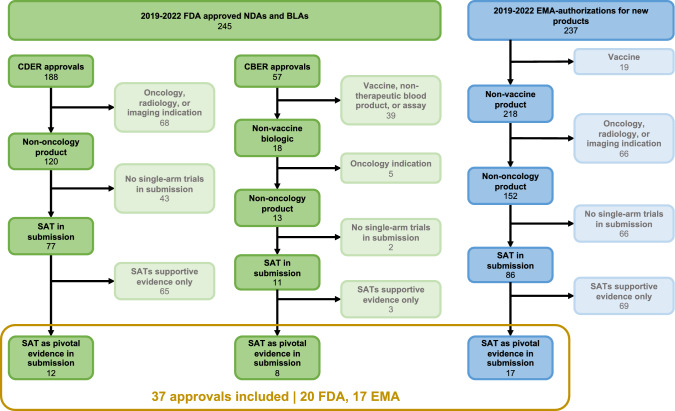
Methods: We examined all non-oncology FDA and EMA drug and biologic approvals for first indications from 2019 to 2022 to identify those with SAT as pivotal safety or efficacy evidence. We abstracted outcomes, key study design features, regulator responses to SAT and (where applicable) ECA design, and product label content.
Results: Among 20 SAT-based FDA approvals and 17 SAT-based EMA approvals, most common indications were progressive rare diseases with high unmet need/limited therapeutic options and a natural history without spontaneous improvement. Of the types of comparators, most were natural history cohorts (45% FDA; 47% EMA) and baseline controls (40% FDA; 47% EMA). Common critiques were of non-contemporaneous ECAs, subjective endpoints, and baseline covariate imbalance between arms.
Conclusion: Based on recent FDA and EMA approvals, the likelihood of regulatory success for SATs with ECAs depends on many design, analytic, and data quality considerations. Our framework is useful in early drug development when considering SAT strategies for evidence generation.
Keywords: External-control-arm; Open-label-studies; Single-arm-trials; Uncontrolled-trials.
© 2024. The Author(s).
Conflict of interest statement
None related to content of manuscript. Authors C.A. and R.P are employed by Takeda Pharmaceuticals and own stock in the company. CERobs Consulting received funding from Takeda Pharmaceuticals for this work. C.G., D.S., R.R., and S.T.T. have no financial interests to disclose.
Figures
References
-
- Joppi R, Bertele’ V, Garattini S. Orphan drugs, orphan diseases. The first decade of orphan drug legislation in the EU. Eur J Clin Pharmacol. 2023. 10.1007/s00228-012-1423-2 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
