

Metabolic modulation to improve MSC expansion and therapeutic potential for articular cartilage repair
- PMID: 39285485
- PMCID: PMC11406821
- DOI: 10.1186/s13287-024-03923-w
Metabolic modulation to improve MSC expansion and therapeutic potential for articular cartilage repair
Erratum in
-
Correction: Metabolic modulation to improve MSC expansion and therapeutic potential for articular cartilage repair.Stem Cell Res Ther. 2024 Nov 7;15(1):403. doi: 10.1186/s13287-024-04048-w. Stem Cell Res Ther. 2024. PMID: 39511618 Free PMC article. No abstract available.
Abstract
Background: Articular cartilage degeneration can result from injury, age, or arthritis, causing significant joint pain and disability without surgical intervention. Currently, the only FDA cell-based therapy for articular cartilage injury is Autologous Chondrocyte Implantation (ACI); however, this procedure is costly, time-intensive, and requires multiple treatments. Mesenchymal stromal cells (MSCs) are an attractive alternative autologous therapy due to their availability and ability to robustly differentiate into chondrocytes for transplantation with good safety profiles. However, treatment outcomes are variable due to donor-to-donor variability as well as intrapopulation heterogeneity and unstandardized MSC manufacturing protocols. Process improvements that reduce cell heterogeneity while increasing donor cell numbers with improved chondrogenic potential during expansion culture are needed to realize the full potential of MSC therapy.
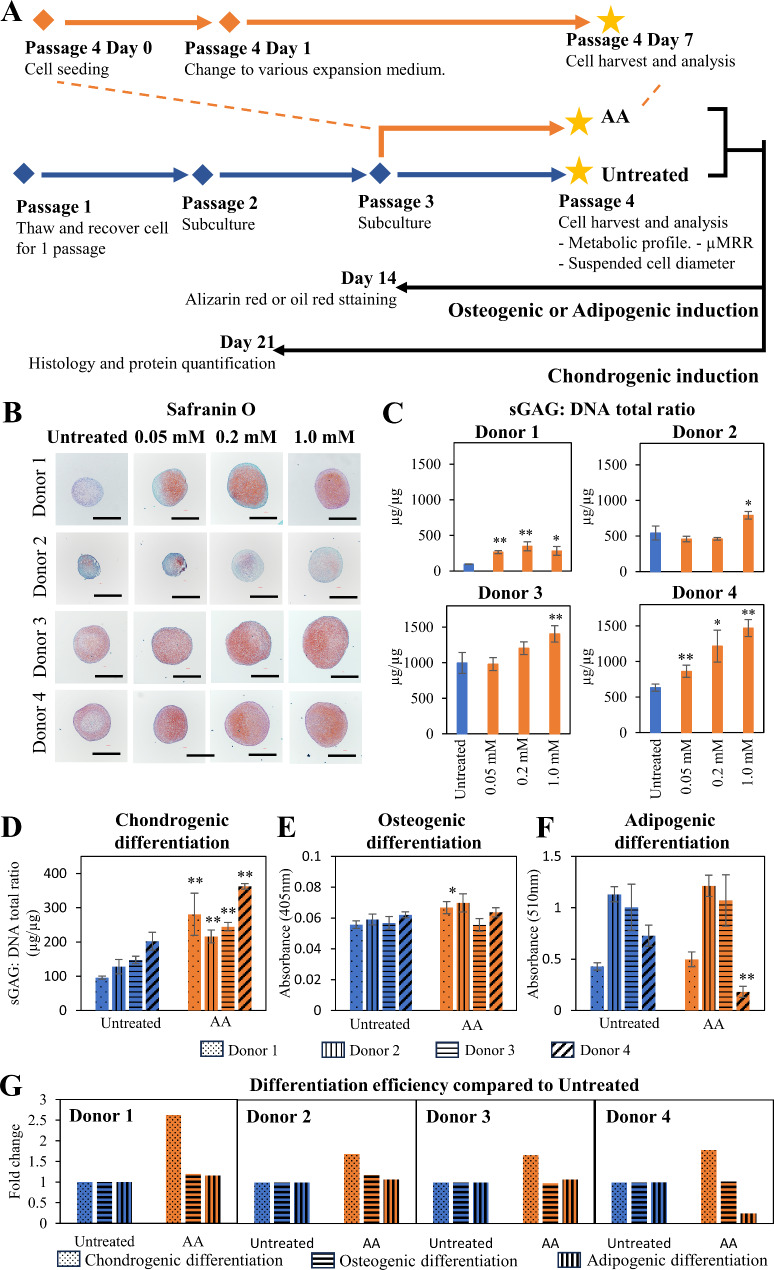
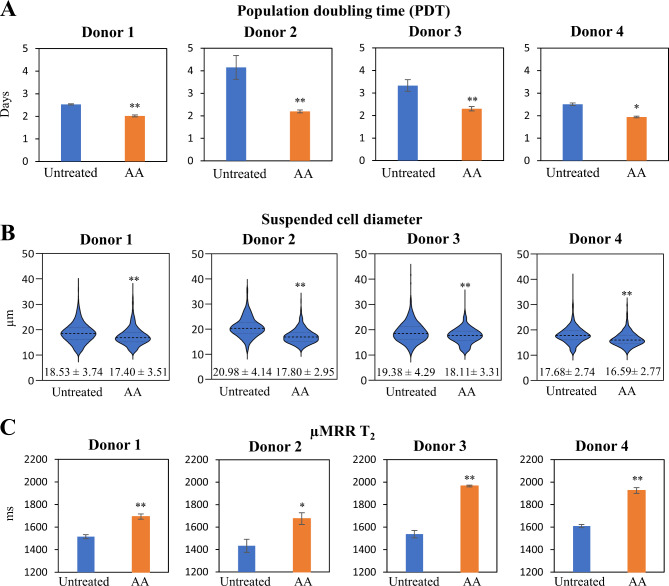
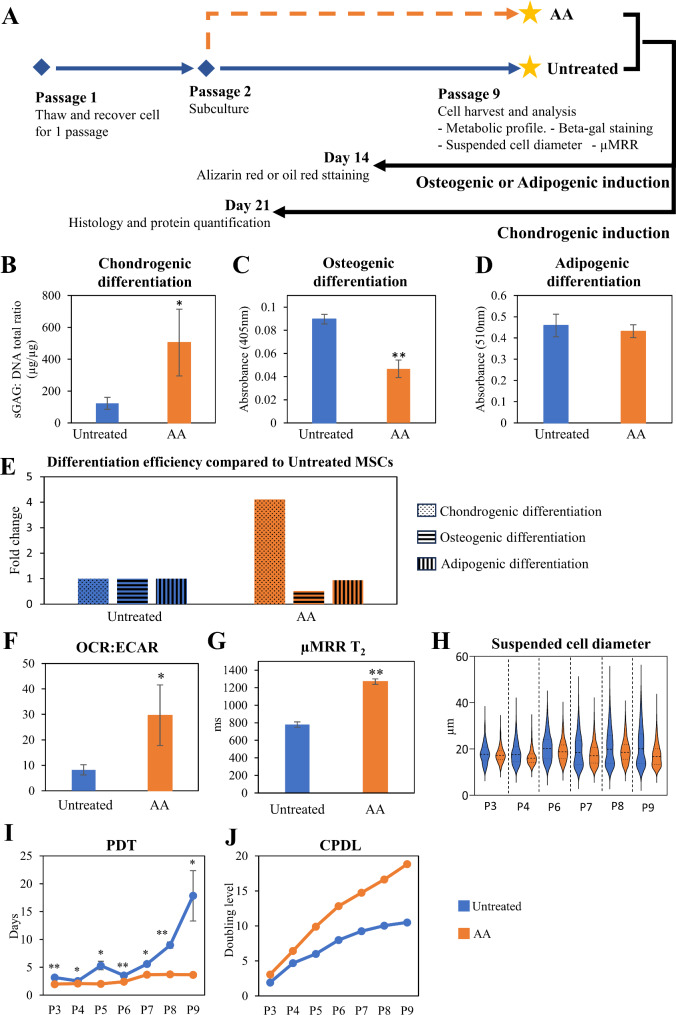
Methods: In this study, we investigated the potential of MSC metabolic modulation during expansion to enhance their chondrogenic commitment by varying the nutrient composition, including glucose, pyruvate, glutamine, and ascorbic acid in culture media. We tested the effect of metabolic modulation in short-term (one passage) and long-term (up to seven passages). We measured metabolic state, cell size, population doubling time, and senescence and employed novel tools including micro-magnetic resonance relaxometry (µMRR) relaxation time (T2) to characterize the effects of AA on improved MSC expansion and chondrogenic potential.
Results: Our data show that the addition of 1 mM L-ascorbic acid-2-phosphate (AA) to cultures for one passage during MSC expansion prior to initiation of differentiation improves chondrogenic differentiation. We further demonstrate that AA treatment reduced the proportion of senescent cells and cell heterogeneity also allowing for long-term expansion that led to a > 300-fold increase in yield of MSCs with enhanced chondrogenic potential compared to untreated cells. AA-treated MSCs with improved chondrogenic potential showed a robust shift in metabolic profile to OXPHOS and higher µMRR T2 values, identifying critical quality attributes that could be implemented in MSC manufacturing for articular cartilage repair.
Conclusions: Our results suggest an improved MSC manufacturing process that can enhance chondrogenic potential by targeting MSC metabolism and integrating process analytic tools during expansion.
Keywords: Articular cartilage; Cell expansion; Critical quality attributes; In-process monitoring tools; Mesenchymal stromal cells; Metabolic modulation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have competing interest.
Figures

References
-
- Nejadnik H, Hui JH, Feng Choong EP, Tai B-C, Lee EH. Autologous bone marrow–derived mesenchymal stem cells versus autologous chondrocyte implantation: an observational cohort study. Am J Sports Med. 2010;38(6):1110–6. - PubMed
-
- Teo AQA, Wong KL, Shen L, Lim JY, Toh WS, Lee EH, et al. Equivalent 10-year outcomes after implantation of autologous bone marrow–derived mesenchymal stem cells versus autologous chondrocyte implantation for chondral defects of the knee. Am J Sports Med. 2019;47(12):2881–7. - PubMed
-
- Wakitani S, Nawata M, Tensho K, Okabe T, Machida H, Ohgushi H. Repair of articular cartilage defects in the patello-femoral joint with autologous bone marrow mesenchymal cell transplantation: three case reports involving nine defects in five knees. J Tissue Eng Regen Med. 2007;1(1):74–9. - PubMed
-
- Maheshwer B, Polce EM, Paul K, Williams BT, Wolfson TS, Yanke A, et al. Regenerative potential of mesenchymal stem cells for the treatment of knee osteoarthritis and chondral defects: a systematic review and meta-analysis. Arthrosc J Arthrosc Relat Surg. 2021;37(1):362–78. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
