

Insights into epidemiological trends of severe chest injuries: an analysis of age, period, and cohort from 1990 to 2019 using the Global Burden of Disease study 2019
- PMID: 39285499
- PMCID: PMC11403847
- DOI: 10.1186/s13049-024-01258-2
Insights into epidemiological trends of severe chest injuries: an analysis of age, period, and cohort from 1990 to 2019 using the Global Burden of Disease study 2019
Abstract
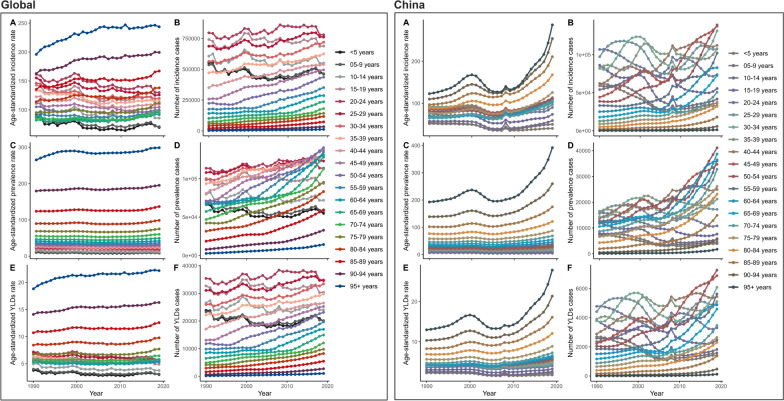
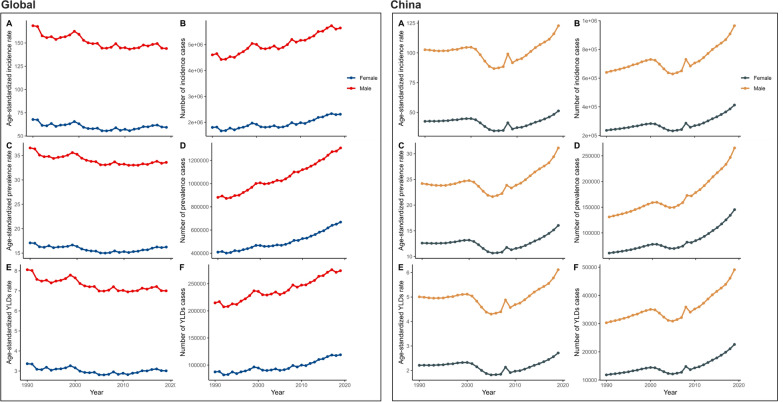
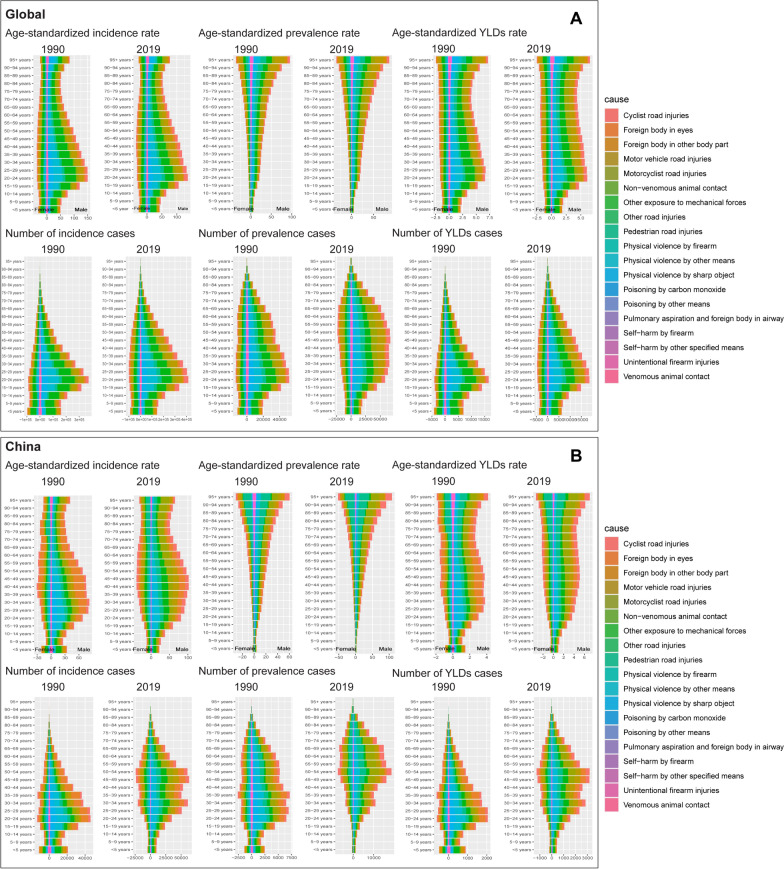
Background: This study assessed the global trends and burden of severe chest injury, including rib fractures, lung contusions, and heart injuries from 1990 to 2019. Herein, we predicted the burden patterns and temporal trends of severe chest injuries to provide epidemiological evidence globally and in China.
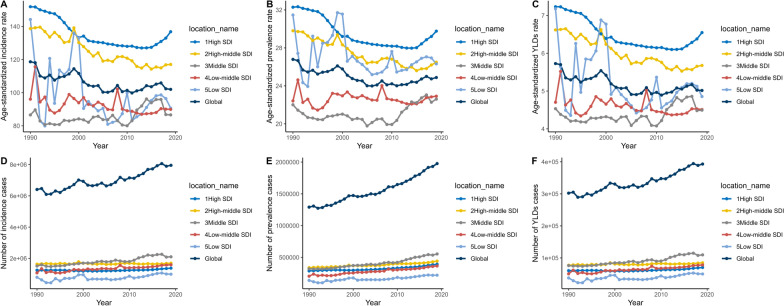
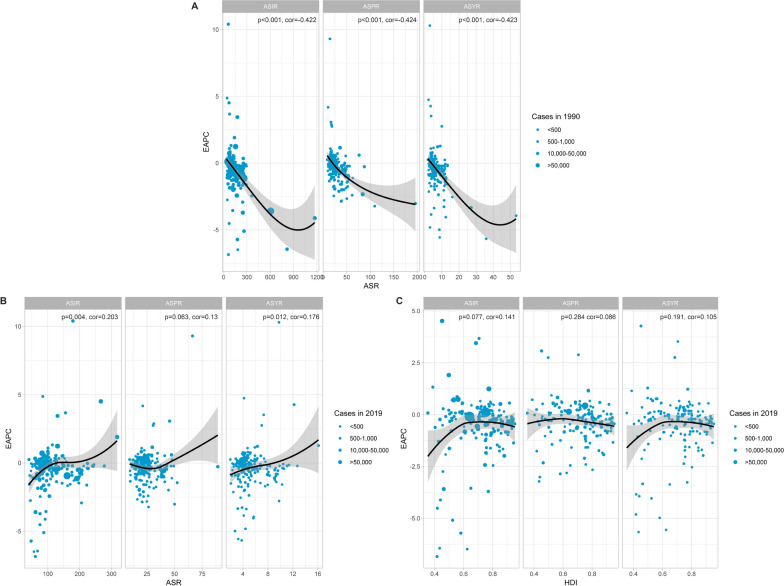
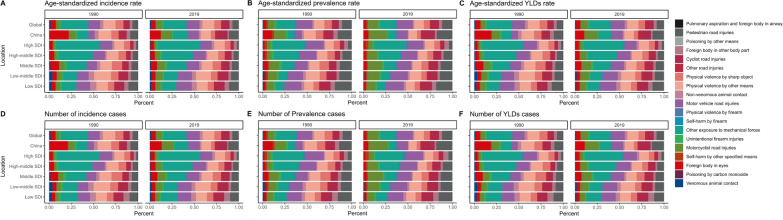
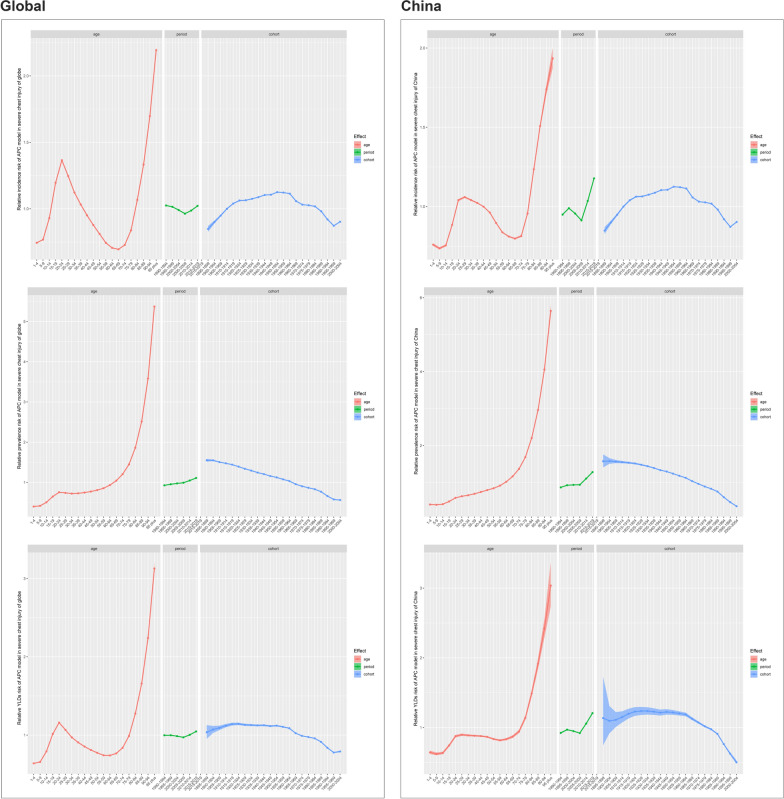
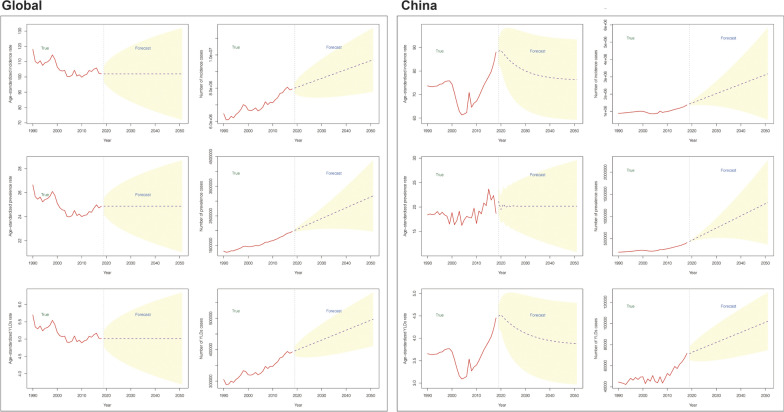
Methods: In our analysis, the age-standardized incidence rate (ASIR), prevalence rate (ASPR), and years lived with disability rate (ASYR) of severe chest injury were analyzed by gender, age, sociodemographic index, and geographical region between 1990 and 2019 using data from the Global Burden of Disease study 2019. Trends were depicted by calculating the estimated annual percentage changes (EAPCs). The impact of age, period, and cohort factors was assessed using an Age-Period-Cohort model. Autoregressive integrated moving average (ARIMA) model was employed to predict severe chest injury trends from 2020 to 2050.
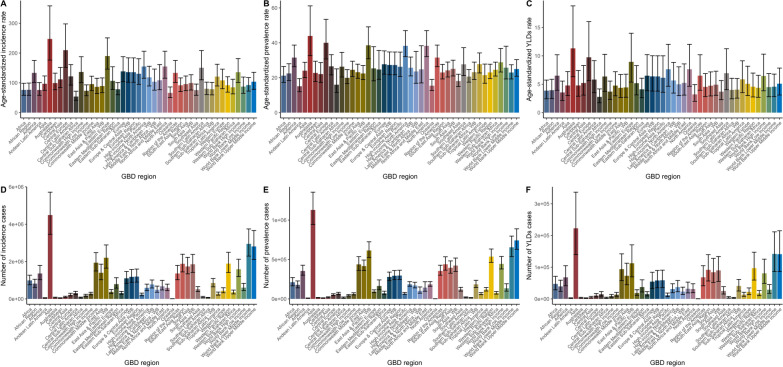
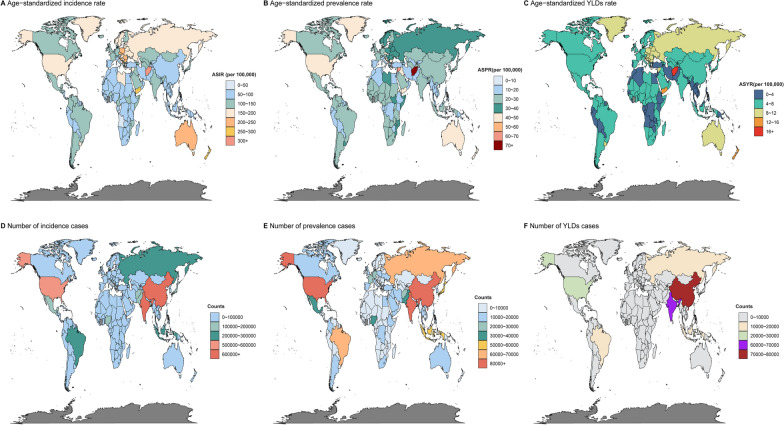
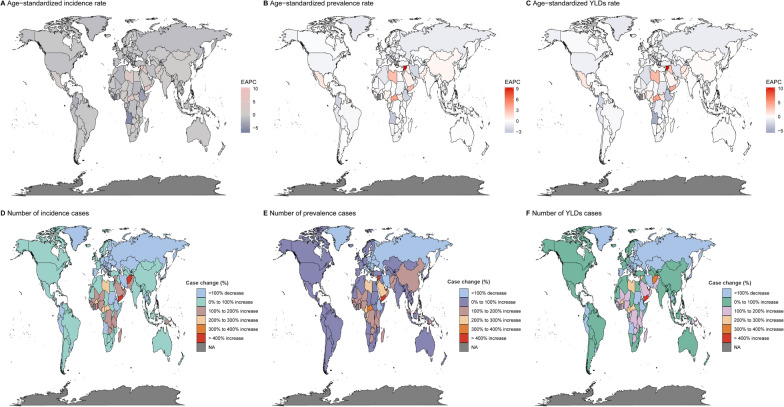
Results: In 2019, the global number of severe chest injury cases reached 7.95 million, with the highest incidence rate observed in Central Europe (209.61). Afghanistan had the highest ASIRs at 277.52, while North Korea had the lowest ASIRs at 41.02. From 1990 to 2019, the Syrian Arab Republic saw significant increases in ASIR, ASPR, and ASYR, with EAPCs of 10.4%, 9.31%, and 10.3%, respectively. Burundi experienced a decrease in ASIR with an EAPC of - 6.85% (95% confidence interval [CI] - 11.11, - 2.37), while Liberia's ASPR and ASYR declined with EAPCs of - 3.22% (95% CI - 4.73, - 1.69) and - 5.67% (95% CI - 8.00, - 3.28), respectively. Falls and road injuries remained the most common causes. The relative risk of severe chest injury by age, period, and cohort demonstrated a complex effect globally and in China. The ARIMA model forecasted a steady increase in global numbers from 2020 to 2050, while in China, it forecasted an increase in incidence, a decrease in ASIR and ASYR, and an increase in ASPR.
Conclusions: This study provides a groundbreaking analysis of global severe chest injury, shedding light on its measures and impact. These findings highlight the need for timely, specialized care and addressing regional disparities to mitigate the severe chest injury burden.
Keywords: ARIMA model; Age-period-cohort; Causes; Global Burden of Disease 2019; Incidence; Prevalence; Severe chest injury; Years lived with disability.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bayer J, Lefering R, Reinhardt S, Kühle J, Südkamp NP, Hammer T. Severity-dependent differences in early management of thoracic trauma in severely injured patients—analysis based on the TraumaRegister DGU®. Scand J Trauma Resusc Emerg Med. 2017;25(1):10. 10.1186/s13049-017-0354-4 - DOI - PMC - PubMed
MeSH terms
Grants and funding
- jjzx2021-gjcsqyylzx01/the Major Research Project of the National Trauma Regional Medical Center (jointly sponsored by the Chongqing Municipal Government and Health Commission
- cstc2022ycjh-bgzxm0245/the Chongqing Elite Research Project
- 2022KFKI07/the open topics of the Key Laboratory of Emergency Medicine in Chongqing
LinkOut - more resources
Full Text Sources
Medical
