

The updated Asia-Pacific consensus statement on the role of endoscopic management in malignant hilar biliary obstruction
- PMID: 39285860
- PMCID: PMC11405119
- DOI: 10.1055/a-2366-7302
The updated Asia-Pacific consensus statement on the role of endoscopic management in malignant hilar biliary obstruction
Abstract
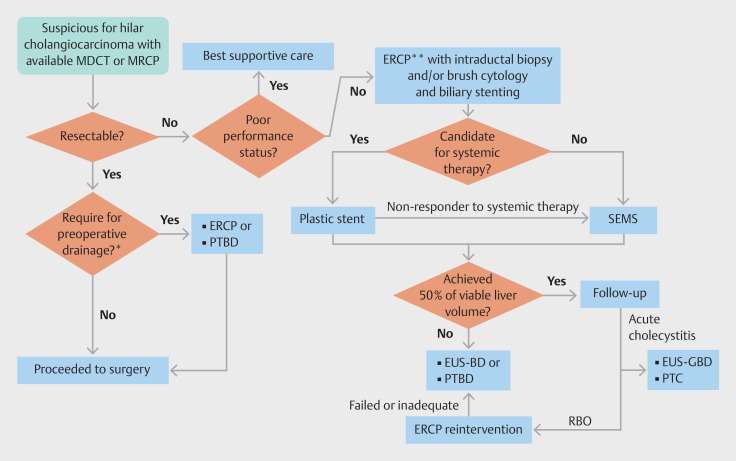
The first Asia-Pacific consensus recommendations for endoscopic and interventional management of hilar cholangiocarcinoma were published in 2013. Since then, new evidence on the role of endoscopy for management of malignant hilar biliary obstruction (MHBO) has emerged. To update the recommendation, we reviewed the literature using a PICO (population/intervention/comparison/outcomes) framework and created consensus statements. The expert panel voted anonymously using the modified Delphi method and all final statements were evaluated for the quality of evidence and strength of recommendation. The important points with inadequate supporting evidence were classified as key concepts. There were seven statements and five key concepts that reached consensus. The statements and key concepts dealt with multiple aspects of endoscopy-based management in MHBO starting from diagnosis, strategies and options for biliary drainage, management of recurrent biliary obstruction, management of cholecystitis after biliary stenting, and adjunctive treatment before stenting. Although the recommendations may assist physicians in planning the treatment for MHBO patients, they should not replace the decision of a multidisciplinary team in the management of individual patients.
Keywords: Biliary tract; ERC topics; Endoscopic ultrasonography; Intervention EUS; Pancreatobiliary (ERCP/PTCD); Strictures; Tissue diagnosis.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest The authors declare that they have no conflict of interest.
Figures
References
-
- Guyatt GH, Oxman AD, Vist GE et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi: 10.1136/bmj.39489.470347.AD. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources