

Association of serum zinc with mineral stress in chronic kidney disease
- PMID: 39286240
- PMCID: PMC11403325
- DOI: 10.1093/ckj/sfae258
Association of serum zinc with mineral stress in chronic kidney disease
Abstract
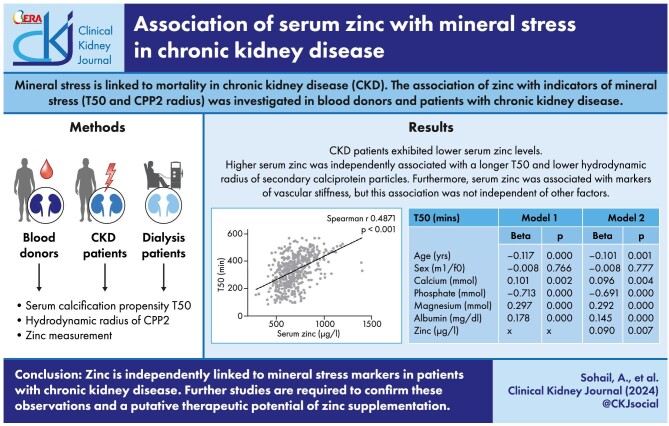
Background: The excessive cardiovascular mortality of patients with chronic kidney disease (CKD) could be linked to mineral stress, the biological consequence of calcium-phosphate nanoparticle exposure. This study investigated whether zinc is associated with mineral stress markers in CKD.
Methods: Zinc and T50 (serum calcification propensity) as well as hydrodynamic radius of secondary calciprotein particles (CPP2) were measured in blood donors and CKD patients with/out dialysis.
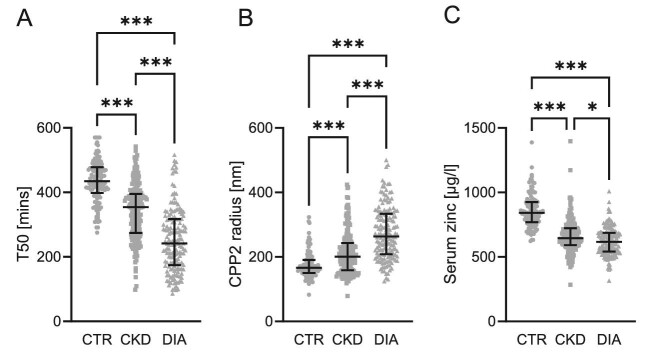
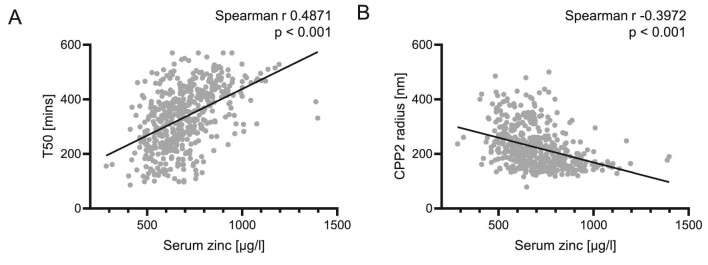
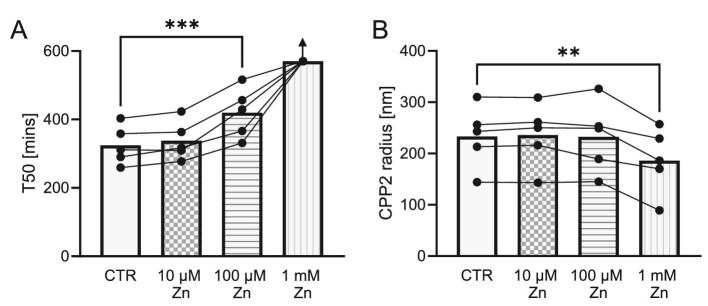
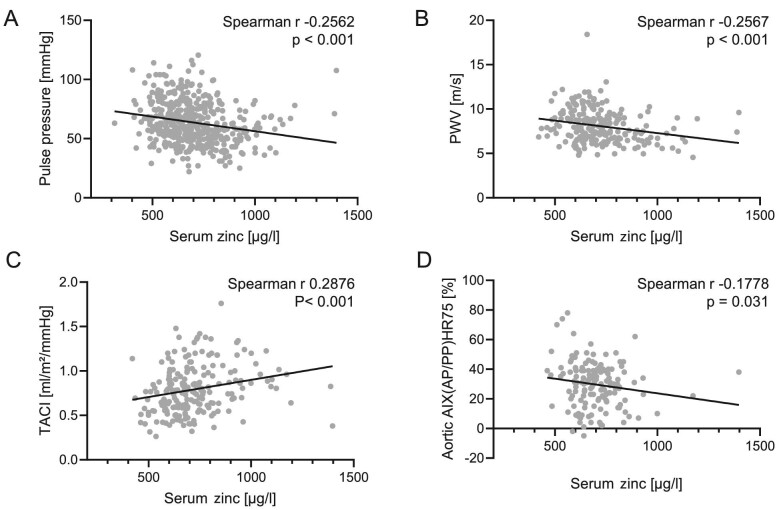
Results: Serum zinc concentrations and T50 were reduced, while CPP2 radius was increased in CKD patients. Serum zinc levels positively correlated with T50 and inversely correlated with CPP2 radius. In a hierarchical linear regression model, T50 was associated with age, calcium, phosphate, magnesium and albumin. Addition of zinc significantly improved prediction of the model, confirming an additional contribution of zinc to T50. Similar observations were made for the association of zinc and CPP2 radius, but spiking experiments indicated that zinc may stronger modify T50 than CPP2 radius. Also, urinary zinc excretion was increased in patients with kidney disease and correlated to T50 and CPP2 radius. Serum zinc further correlated with markers of arterial stiffness in blood donors and CKD patients, but these associations did not remain significant in a multivariate linear regression model.
Conclusions: Reduced serum zinc levels in CKD appear directly linked to lower T50 and associated with larger CPP2 radius. Further studies on the associations of zinc and mineral stress as well as putative therapeutic benefits of zinc supplementation are required.
Keywords: calciprotein particles; chronic kidney disease; mineral stress; serum calcification propensity; zinc.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
A.P. is stockholder of Calciscon AG (Biel, Switzerland), which commercializes the mineral stress analysis used in this study.
Figures
References
LinkOut - more resources
Full Text Sources
