

Ultra-processed foods and cardiovascular disease: analysis of three large US prospective cohorts and a systematic review and meta-analysis of prospective cohort studies
- PMID: 39286398
- PMCID: PMC11403639
- DOI: 10.1016/j.lana.2024.100859
Ultra-processed foods and cardiovascular disease: analysis of three large US prospective cohorts and a systematic review and meta-analysis of prospective cohort studies
Abstract
Background: Prospective associations between total and groups of ultra-processed foods (UPF) and cardiovascular disease (CVD) remained to be characterised. Our aim was to assess the association of total and group-specific UPF intakes with CVD, coronary heart disease (CHD), and stroke in three large prospective cohorts of US adults. Additionally, we conducted a systematic review and meta-analyses on the existing evidence on the associations of total UPF intake with these outcomes.
Methods: UPF intake was assessed through food frequency questionnaires in the Nurses' Health Study (NHS; n = 75,735), Nurses' Health Study II (NHSII; n = 90,813), and Health Professionals Follow-Up Study (HPFS; n = 40,409). Cox regression estimated cohort-specific associations of total and group-specific UPF intake with risk of CVD (cases = 16,800), CHD (cases = 10,401), and stroke (cases = 6758), subsequently pooled through fixed-effect models. Random-effects meta-analyses pooled existing prospective findings on the UPF-CVD association identified on Medline and Embase up to April 5, 2024, without language restrictions. Risk of bias was assessed with the Newcastle-Ottawa Scale, funnel plots, and Egger's tests, and meta-evidence was evaluated using NutriGrade.
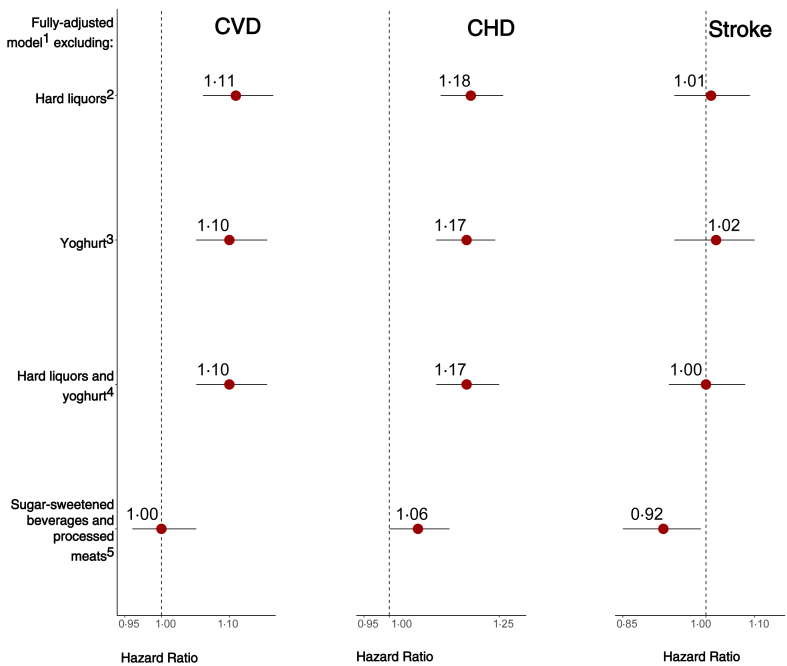
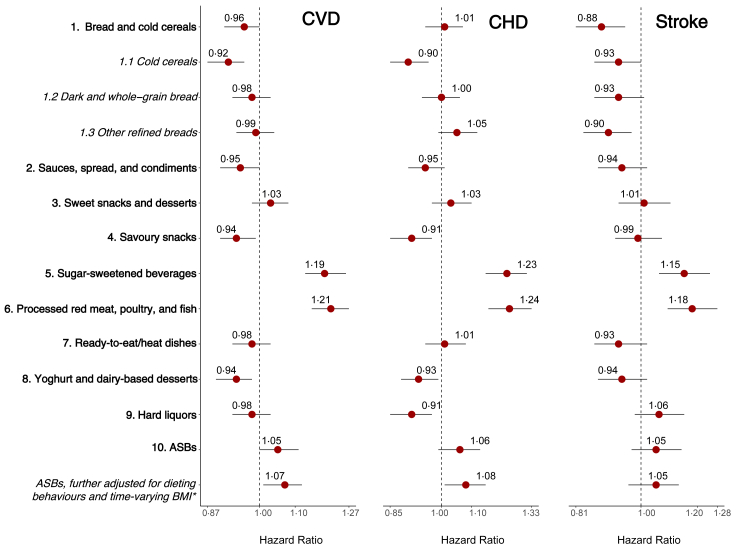
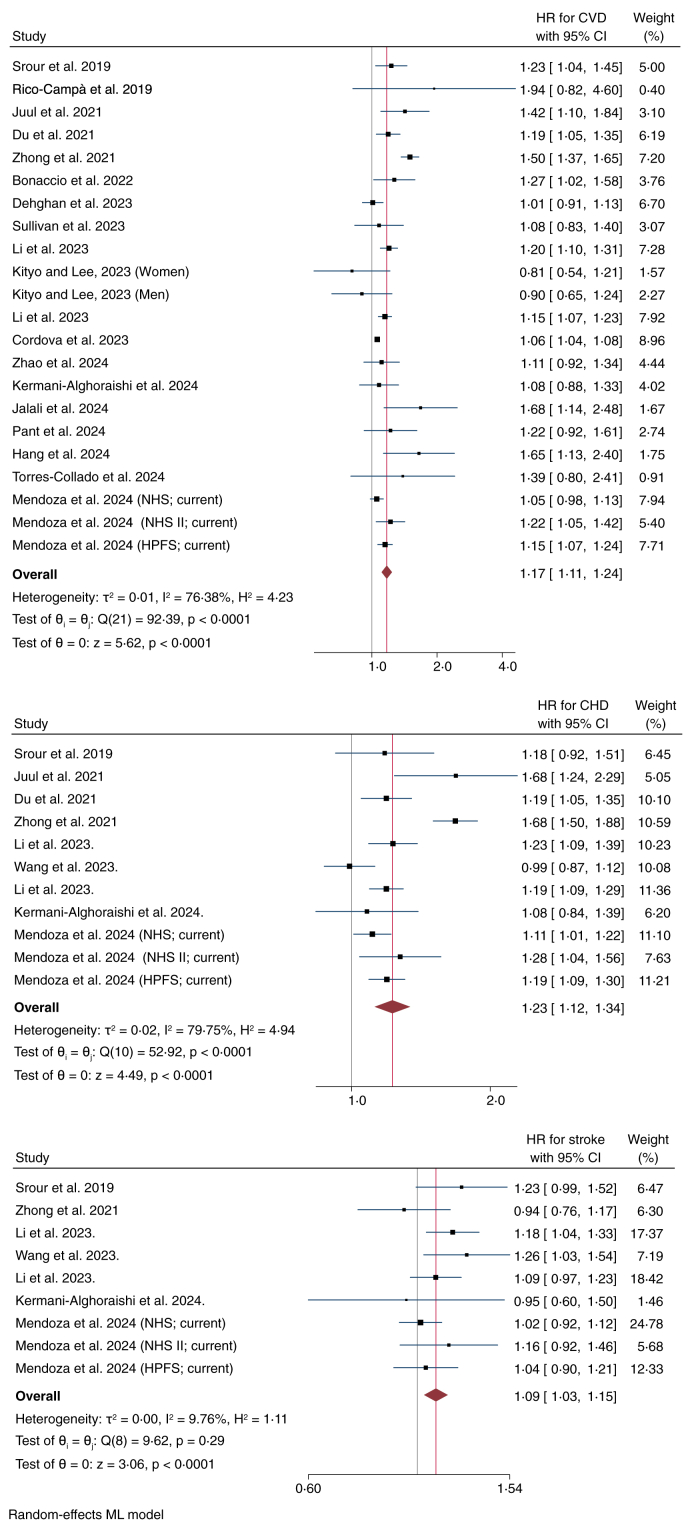
Findings: The baseline mean (SD) age was 50.8 years (7.2) for the NHS, 36.7 years (4.6) for the NHSII, and 53.4 years (9.6) for the HPFS. The proportion of participants of White race was 97.7% in the NHS, 96.4% in the NHSII, and 94.9% in the HPFS. Among the three cohorts, multivariable-adjusted hazard ratios [HRs (95% CIs)] for CVD, CHD, and stroke for the highest (vs. lowest) total UPF intake quintile were 1.11 (1.06-1.16), 1.16 (1.09-1.24), and 1.04 (0.96-1.12), respectively. UPF groups demonstrated divergent associations. Sugar-/artificially-sweetened drinks and processed meats were associated with higher CVD risk, whereas inverse associations were observed for bread/cold cereals, yoghurt/dairy desserts, and savoury snacks. Meta-analysing 22 prospective studies showed that total UPF intake at the highest category (vs. lowest) was associated with 17% (11%-24%), 23% (12%-34%), and 9% (3%-15%) higher CVD, CHD, and stroke risk. Meta-evidence quality was high for CHD, moderate for CVD, and low for stroke.
Interpretation: Total UPF intake was adversely associated with CVD and CHD risk in US adults, corroborated by prospective studies from multiple countries, also suggesting a small excess stroke risk. Nutritional advice for cardiovascular health should consider differential consequences of group-specific UPF. Replication is needed in racially/ethnically-diverse populations.
Funding: National Institutes of Health (NIH) grants supported the NHS, NHSII, and HPFS.
Keywords: Cardiovascular disease; Cohort studies; Meta-analysis; Nurses’ health study; Systematic analysis; Ultra-processed foods.
© 2024 The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
