

Real-world impact of transitioning from one lipoprotein(a) assay to another in a clinical setting
- PMID: 39286651
- PMCID: PMC11402909
- DOI: 10.1016/j.ajpc.2024.100726
Real-world impact of transitioning from one lipoprotein(a) assay to another in a clinical setting
Abstract
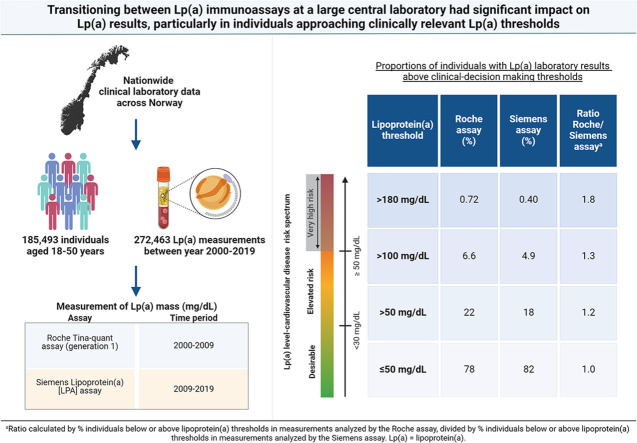
Background and aims: Different lipoprotein(a) [Lp(a)] assays may affect risk stratification of individuals and thus clinical decision-making. We aimed to investigate how transitioning between Lp(a) assays at a large central laboratory affected the proportion of individuals with Lp(a) result above clinical thresholds.
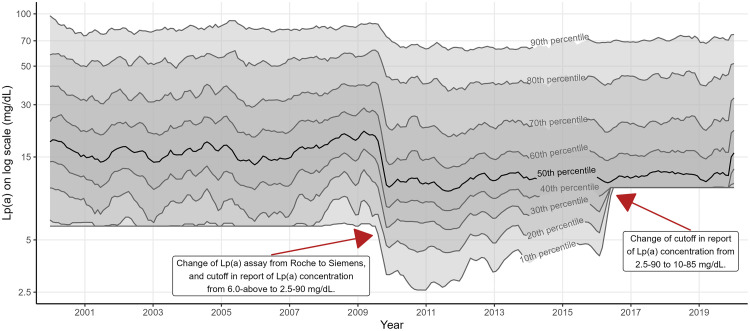
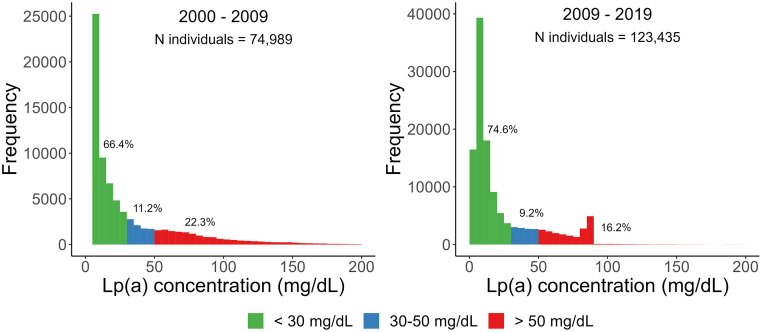
Methods: We studied nationwide clinical laboratory data including 185,493 unique individuals (47.7 % women) aged 18-50 years with 272,463 Lp(a) measurements using Roche (2000-2009) and Siemens Lp(a) assay (2009-2019).
Results: While the majority of individuals (66-75 %) had low levels of Lp(a) (<30 mg/dL) independent of the assay used, the Roche assay detected 20 % more individuals with Lp(a) >50 mg/dL, 40 % more individuals with Lp(a) >100 mg/dL and 80 % more individuals with Lp(a) > 180 mg/dL than the currently used Siemens assay, likely due to calibration differences.
Conclusion: Transitioning from one Lp(a) immunoassay to another had significant impact on Lp(a) results, particularly in individuals approaching clinically relevant Lp(a) thresholds.
Keywords: Lipids; Lipoprotein(a); Lipoprotein(a) assay.
© 2024 The Authors.
Conflict of interest statement
Jeevanathan has received consultancy fees from Novartis, and had a part time student internship at Novartis organized by the Faculty of Medicine at University of Oslo and the Student Association for Medical Innovation prior to this study. Dr. Blom is an employee of Novartis Norway AS. Dr. Nordestgaard has had consultancies or talks sponsored by Abbott, Akcea, Amarin, Amgen, AstraZeneca, Denka, Esperion, Kowa, Lilly, Mankind, Novartis, Novo Nordisk, Regeneron, Sanofi, Silence Therapeutics, Ultragenyx, and USV. Dr. Retterstøl has received personal fees from Amgen, Mills AS, The Norwegian Medical Association, The Norwegian Directorate of Health, Sanofi, Novo Nordisk, none of which are related to the content of this manuscript. The other authors have no financial relationships relevant to disclose.
Figures
References
-
- Kronenberg F., Mora S., Stroes E.S.G., Ference B.A., Arsenault B.J., Berglund L., et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022;43:3925–3946. doi: 10.1093/eurheartj/ehac361. - DOI - PMC - PubMed
-
- Dati F., Tate J.R, Marcovina S.M., Steinmetz A. International federation of clinical chemistry and laboratory medicine, IFCC Working Group for Lipoprotein(a) Assay Standardization. First WHO/IFCC international reference reagent for lipoprotein(a) for immunoassay–Lp(a) SRM 2B. Clin Chem Lab Med. 2004;42:670–676. doi: 10.1515/CCLM.2004.114. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
