

External validation of a deep learning model for automatic segmentation of skeletal muscle and adipose tissue on abdominal CT images
- PMID: 39286936
- PMCID: PMC11573127
- DOI: 10.1093/bjr/tqae191
External validation of a deep learning model for automatic segmentation of skeletal muscle and adipose tissue on abdominal CT images
Abstract
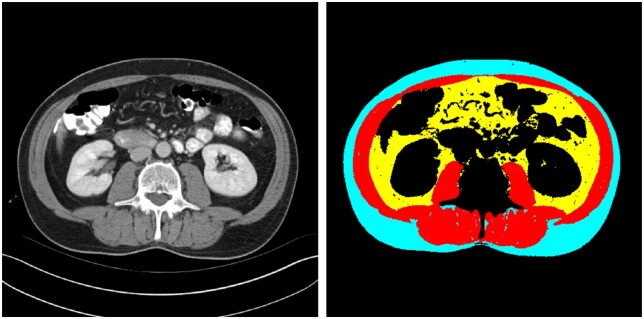
Objectives: Body composition assessment using CT images at the L3-level is increasingly applied in cancer research and has been shown to be strongly associated with long-term survival. Robust high-throughput automated segmentation is key to assess large patient cohorts and to support implementation of body composition analysis into routine clinical practice. We trained and externally validated a deep learning neural network (DLNN) to automatically segment L3-CT images.
Methods: Expert-drawn segmentations of visceral and subcutaneous adipose tissue (VAT/SAT) and skeletal muscle (SM) of L3-CT-images of 3187 patients undergoing abdominal surgery were used to train a DLNN. The external validation cohort was comprised of 2535 patients with abdominal cancer. DLNN performance was evaluated with (geometric) dice similarity (DS) and Lin's concordance correlation coefficient.
Results: There was a strong concordance between automatic and manual segmentations with median DS for SM, VAT, and SAT of 0.97 (IQR: 0.95-0.98), 0.98 (IQR: 0.95-0.98), and 0.95 (IQR: 0.92-0.97), respectively. Concordance correlations were excellent: SM 0.964 (0.959-0.968), VAT 0.998 (0.998-0.998), and SAT 0.992 (0.991-0.993). Bland-Altman metrics indicated only small and clinically insignificant systematic offsets; SM radiodensity: 0.23 Hounsfield units (0.5%), SM: 1.26 cm2.m-2 (2.8%), VAT: -1.02 cm2.m-2 (1.7%), and SAT: 3.24 cm2.m-2 (4.6%).
Conclusion: A robustly-performing and independently externally validated DLNN for automated body composition analysis was developed.
Advances in knowledge: This DLNN was successfully trained and externally validated on several large patient cohorts. The trained algorithm could facilitate large-scale population studies and implementation of body composition analysis into clinical practice.
Keywords: CT; body composition; convolutional neural networks; deep learning; image segmentation.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology.
Conflict of interest statement
None declared.
Figures


References
-
- Mourtzakis M, Prado CMM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE.. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. 2008;33(5):997-1006. - PubMed
-
- Martin L, Birdsell L, Macdonald N, et al.Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. 2013;31(12):1539-1547. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
