

Pressure control plus spontaneous ventilation versus volume assist-control ventilation in acute respiratory distress syndrome. A randomised clinical trial
- PMID: 39287651
- PMCID: PMC11457688
- DOI: 10.1007/s00134-024-07612-3
Pressure control plus spontaneous ventilation versus volume assist-control ventilation in acute respiratory distress syndrome. A randomised clinical trial
Abstract
Purpose: The aim of this study was to compare the effect of a pressure-controlled strategy allowing non-synchronised unassisted spontaneous ventilation (PC-SV) to a conventional volume assist-control strategy (ACV) on the outcome of patients with acute respiratory distress syndrome (ARDS).
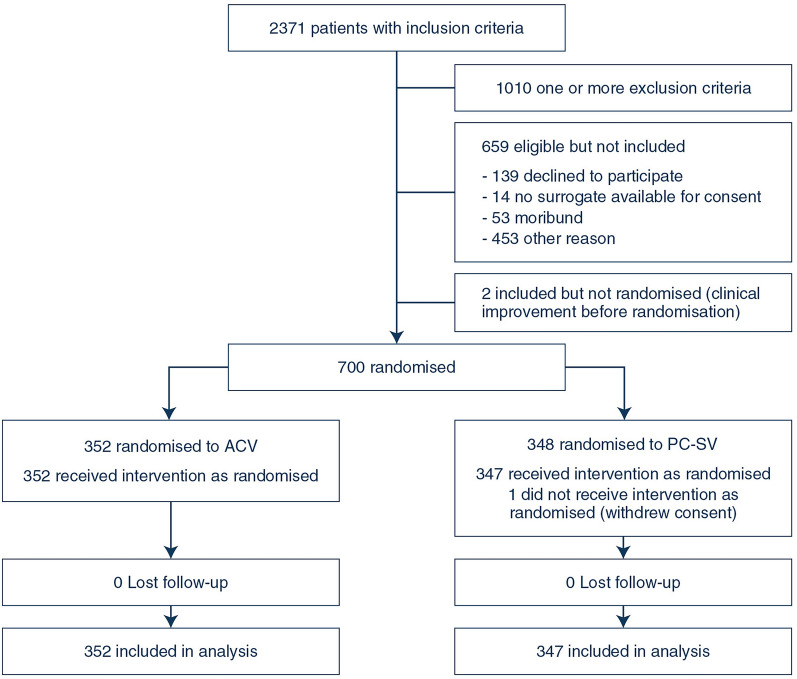
Methods: Open-label randomised clinical trial in 22 intensive care units (ICU) in France. Seven hundred adults with moderate or severe ARDS (PaO2/FiO2 < 200 mmHg) were enrolled from February 2013 to October 2018. Patients were randomly assigned to PC-SV (n = 348) or ACV (n = 352) with similar objectives of tidal volume (6 mL/kg predicted body weight) and positive end-expiratory pressure (PEEP). Paralysis was stopped after 24 h and sedation adapted to favour patients' spontaneous ventilation. The primary endpoint was in-hospital death from any cause at day 60.
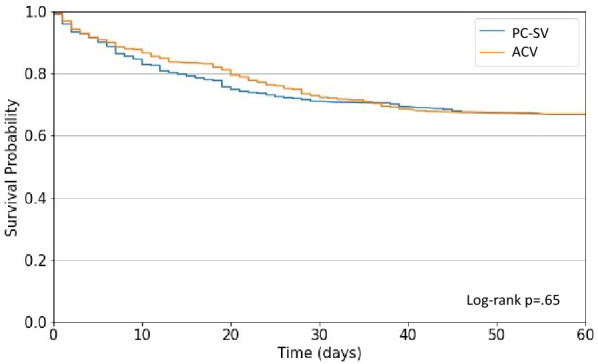
Results: Hospital mortality [34.6% vs 33.5%, p = 0.77, risk ratio (RR) = 1.03 (95% confidence interval [CI] 0.84-1.27)], 28-day mortality, as well as the number of ventilator-free days and organ failure-free days at day 28 did not differ between PC-SV and ACV groups. Patients in the PC-SV group received significantly less sedation and neuro-muscular blocking agents than in the ACV group. A lower proportion of patients required adjunctive therapy of hypoxemia (including prone positioning) in the PC-SV group than in the ACV group [33.1% vs 41.3%, p = 0.03, RR = 0.80 (95% CI 0.66-0.98)]. The incidences of pneumothorax and refractory hypoxemia did not differ between the groups.
Conclusions: A strategy based on PC-SV mode that favours spontaneous ventilation reduced the need for sedation and adjunctive therapies of hypoxemia but did not significantly reduce mortality compared to ACV with similar tidal volume and PEEP levels.
Keywords: Acute respiratory distress syndrome; Mechanical ventilation; Neuro-muscular blocking agents; Pressure-controlled ventilation; Sedation; Spontaneous ventilation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare having no potential conflict of interest relevant to the present manuscript.
Figures
References
-
- Dres M, Dubé B-P, Mayaux J et al (2017) Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med 195:57–66. 10.1164/rccm.201602-0367OC - PubMed
-
- Richard JCM, Lyazidi A, Akoumianaki E et al (2013) Potentially harmful effects of inspiratory synchronization during pressure preset ventilation. Intensive Care Med 39:2003–2010. 10.1007/s00134-013-3032-7 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
